Outcomes of NC Medical School Graduates: How Many Stay in Practice in NC, in Primary Care, and in High Need Areas?
By Evan Galloway, Hugh H. Tilson Jr.
Apr 11, 2025
Executive Summary
In 1993, the General Assembly mandated an annual report on the number of North Carolina (NC) medical school graduates going into primary care. Since 1994, the Cecil G. Sheps Center for Health Services Research at the University of North Carolina at Chapel Hill (“Sheps Center”) andthe NC Area Health Education Centers program (AHEC) have collaborated to produce this report which tracks the number of students practicing primary care in rural NC five years after graduation from an NC medical school. As a result of the legislative mandate, NC is a national model for tracking medical student outcomes.
As in prior years, this report tracks NC medical school graduate outcomes for physicians who practice in NC and in rural NC counties. This report includes all five medical schools in North Carolina, both public and private. The Campbell School of Osteopathic Medicine graduated its first class in 2017, so they are not included in the 2014 cohort. This report also includes an analysis of the number of medical school graduates that practice in NC safety net settings1 that deliver care to uninsured, Medicaid, and other vulnerable populations, a description in Appendix A of each medical school’s efforts to increase the number of graduates practicing primary care in rural NC and a description in Appendix B of on-going efforts to establish a defined “Pathway to Primary Care” in NC.
Historically, this report examined NC medical school graduates five years following graduation per the legislative mandate. However, this period is not ideal because the time required to complete residency after medical school graduation ranges from three to more than six years. At five-years post-graduation from medical school, physicians in psychiatry, obstetrics & gynecology (ob/gyn), surgery, and medicine/pediatrics are just completing residency, or may be in fellowship/specialty training, and may not have settled in a permanent practice location. Thus, although not required by the legislature, this report also includes ten-year outcomes for the 2014 cohort.
When reviewing this report, it is important to keep in mind that North Carolina’s medical schools represent just one component in shaping the size and composition of our physician workforce. Physicians’ decisions about specialty choice and practice location are shaped by numerous other factors including the availability and location of residency training programs in needed specialties and geographies, loan repayment, compensation and life-style factors.
Analyses of the five-year outcomes of NC class of 2019 graduates and ten-year outcomes of NC class of 2014 graduates show:
- Of the 628 NC medical school graduates from the class of 2019, 62 (10%) were in practice or training in primary care in NC in 2024, and 5 (<1%) are in primary care in a rural NC county.
- Of the 446 NC medical school graduates from the class of 2014, 56 (13%) were practicing primary care in NC in 2024, 10 years post-graduation and 11 graduates (2.5%) were in rural primary care in NC.
- Both UNC and ECU retained the largest proportion of graduates in practice or training in NC in any specialty after five years (46% and 38%, respectively), followed by Duke (24%), Campbell (21%), Wake Forest (18%).
- UNC and ECU had the largest proportions of graduates practicing in primary care in NC five years after graduating in 2019 (17% and 15%, respectively). From this cohort, UNC contributed 29 graduates to the state primary care workforce, while Campbell contributed 14 and ECU added 11.
- Across both the 2014 and 2019 cohorts, 13 graduates were found to be practicing or training in a safety net setting.1
- Three percent (19/628) of the class of 2019 and nearly five percent (21/446) of the class of 2014 worked in a practice location in the most economically distressed neighborhoods in NC five and ten years, respectively, after graduation.
- Twelve 2014 graduates were in practice in general surgery in NC ten years after graduating with one in a rural county. Five graduates from the same year were practicing psychiatry in NC ten years later with none practicing primarily in a rural county.
Background
In 1993, the North Carolina General Assembly expressed interest in expanding the pool of generalist physicians (i.e., primary care physicians) for the state. To increase the supply, as part of N.C.S.L.1993-321 the General Assembly required each of the state’s four medical schools to develop a plan to expand the percent of medical school graduates choosing residency positions in primary care. Primary care was defined as family practice, general internal medicine, general pediatric medicine, internal medicine-pediatrics, and obstetrics-gynecology. It set the goal for East Carolina University (ECU) and UNC Schools of Medicine at 60% of graduates entering primary care. For the Wake Forest University and Duke University Schools of Medicine, it set the goal at 50%. Campbell University School of Osteopathic Medicine graduated its first class in 2017 and was therefore not included in these original goals.
Since 1994, the Cecil G. Sheps Center for Health Services Research at the University of North Carolina at Chapel Hill (“Sheps Center”) and the NC Area Health Education Centers program (AHEC) have collaborated to produce this report tracks the workforce outcomes for NC medical schools. As a result of the legislative mandate, NC is a national model for tracking medical student outcomes. Data from this report were featured in the New England Journal of Medicine as an example of how to track workforce outcomes in John Iglehart’s 2018 article on “The challenging quest to improve rural health care.“2
While not required by the original legislation, the Sheps Center and NC AHEC have enhanced the annual report to better reflect the state’s workforce needs. As in prior years, this report tracks NC medical school graduate outcomes for physicians who practice in NC and in rural NC counties. However, this report also includes an analysis of the number of medical school graduates that practice in NC safety net settings1 and in areas of high economic deprivation in NC. We have also included an analysis of graduates retained in psychiatry and general surgery in NC.
Historically, this report has examined NC medical school graduates at five years following graduation per the legislative mandate. However, this period is not ideal because the time required to complete residency after graduation from medical school ranges between three to six years or more. At five-years post-graduation from medical school, physicians in psychiatry, obstetrics & gynecology (ob/gyn), surgery, and medicine/pediatrics are just completing residency, or may be in fellowship/specialty training, and may not have settled in a permanent practice location. This is typically the case for general surgeons, whose training period is five years, and for ob/gyns, psychiatrists and medicine/pediatrics residents who often do a fellowship after a four-year residency. Ten years following graduation from medical school is a more reasonable timeframe to track outcomes, as it allows for fellowship training following residency. Thus, although not required by the legislature, this report also includes ten-year outcomes for the 2014 cohort.
Since reporting on medical student outcomes began in 1994, Campbell University became the fifth medical school in North Carolina and is included in this report. The health care system has also undergone dramatic change in in the last thirty years and the data in this report remain as critical as ever to help inform the state’s efforts to address chronic shortfalls of primary care physicians, especially in rural areas. The composition of the primary care workforce itself has also changed. For example, an increasing proportion of general internal medicine physicians are subspecializing; recent national analyses found the percentage of graduating internal medicine residents planning a career in general internal medicine has declined by half in the last decade.3 Concurrently, the growth of hospitalists and the declining number of internal medicine physicians trained, and practicing, in community-based settings has reduced the number of primary care physicians choosing community-based primary care medicine.
Data Sources and Methods
Data Sources
Data included in this report come from several sources:
- The North Carolina Medical Board’s annual licensure files (NCMB), maintained by the NC Health Professions Data System at the Cecil G. Sheps Center for Health Services Research
- GMETrack, the graduate medical education tracking file of the Association of American Medical Colleges (AAMC)
- Data from the alumni and student affairs offices at the Campbell University School of Osteopathic Medicine, the Duke University School of Medicine, the Brody School of Medicine at East Carolina University, the University of North Carolina at Chapel Hill School of Medicine, and the Wake Forest University School of Medicine
- The Federal Office of Management and Budget (OMB) for population and core based statistical area data, which are used to determine which counties in NC are classified as metropolitan (urban) or non-metropolitan (rural). For this report, we used the July 2023 file in which 55 counties in North Carolina are rural (non-metropolitan).
- The 2010 Rural-Urban Commuting Area (RUCA) codes for US census tracts in North Carolina from the US Department of Agriculture’s Economic Research Service. Census tracts with scores of 4 or greater were considered rural, even if their county was metropolitan. This is similar to the methodology of the Federal Office of Rural Health Policy.
- The NC Department of Health and Human Services (DHHS) list of safety net sites, updated in July 2024.
- The 2022 vintage of the Area Deprivation Index (ADI) produced by the University of Wisconsin Center for Health Disparities Research. We used the version of the index which is calculated relative only to areas within the state, not the entire nation.
Campbell University School of Osteopathic Medicine (Campbell) is not mandated to provide data for this report, as the school did not exist when the 1993 legislation was passed. However, Campbell has provided initial match data for the last several years and now has its third fiveyear cohort reported in this report.
As in prior years, this report does not emphasize the data from initial residency matches because many physicians change residency specialties, subsequently subspecialize, or change geographic location over the course of their GME training. For this reason, workforce outcomes are better measured after residency training and a report on those outcomes is forthcoming.
Methods
We merged GMETrack data from the AAMC for 2014 and 2019 medical school graduates with the 2024 NCMB annual licensure file (housed with the Health Professions Data System) to determine physician practice outcomes at five or ten years post-graduation from medical school. The NCMB’s licensure data provides in-state practice locations and areas of practice, while the GMETrack data from the Association of American Medical Colleges (AAMC) is the source list for graduates within a cohort. This is consistent with the methodology of this report for most of its existence; however, we used a different methodology in the last two years to account for an interruption in our access to the AAMC data.
Primary care residency specialties are defined by legislation passed by the NC General Assembly in 1993 (Senate Bill 27/ House Bill 729) and include family medicine, general internal medicine, general pediatric medicine, internal medicine-pediatrics, and obstetrics and gynecology. Even though internal medicine-pediatrics is not reported as an area of practice by the NCMB, physicians trained in internal medicine-pediatrics typically report either pediatrics or general internal medicine as an area of practice and are therefore still captured as primary care physicians in the report.
“Primary Care” is defined for both initial specialty of residency training (identified in GMETrack data for each cohort) and for current practice or training area (identified using NCMB data for physicians in NC). As discussed above, many graduates who initially match to internal medicine and are counted as primary care for their initial match to residency training will go onto train and practice in subspecialties outside of primary care five years after graduation. Asa result, the number of medical students matching to primary care for their initial residency choice is overstated relative to the number of physicians who will end up practicing in primary care.
Psychiatry includes physicians who report practicing in the following specialties: Psychiatry, Child and Adolescent Psychiatry, Psychoanalysis, Forensic Psychiatry, Psychosomatic Medicine, Psychiatry/Geriatric, Family Medicine-Psychiatry, Internal Medicine-Psychiatry, and PediatricsPsychiatry.
General surgery includes physicians report practicing in the following specialties: General Surgery, Abdominal Surgery, Colon & Rectal Surgery, Critical Care Surgery, Head and Neck Surgery, Oncology Surgery, Pediatric Surgery, Transplant Surgery, Trauma Surgery, or Vascular Surgery.
For safety net provider information, we geocoded both the North Carolina Department of Health and Human Services safety net site list and the practice addresses in the NCMB file for each cohort. We then intersected the geocoded datasets to find potential matches between providers and sites. Potential matches were manually checked for accuracy. Safety net providers are defined as health care facilities that provide a significant level of health care and other health-related services to uninsured, Medicaid, and other vulnerable populations. These include rural health clinics, rural health centers, federally qualified health centers, free and charitable clinics, small rural hospitals, health departments, and critical access hospitals. We also used the geocoded locations to place each physician in a block group and a county, allowing us to assign each to an area deprivation index and non-metropolitan (rural) status.
The Area Deprivation Index (ADI) is a measure that summarizes the socioeconomic distress of a Census block group using data from the American Community Survey.i The ADI is based on factors related to income, education, employment, and housing quality in a census block group, which is the geographic equivalent of a neighborhood, The index uses 17 different measurements across a range of domains, like “Percent of households without a motor vehicle” and “Percent of population aged >= 25 years with < a high school diploma”. The weights from a factor analysis of these variables are used to calculate a score for each block group, which is then converted to a decile ranking for each block group relative to the other block groups in the state.
To define rural in this report, we use the US Census Bureau and US OMB’s July 2023 “Core Based Statistical Area” (CBSA) delineations and 2010 RUCA codes. In this analysis, nonmetropolitan counties include micropolitan and counties outside of CBSAs, as well as census tracts with a RUCA score of 4 or greater. The use of RUCA codes in this year’s report expands the number of areas considered rural because it includes rural Census tracts in metropolitan counties, and more closely follows the methodology of the Federal Office of Rural Health.
To report initial residency match data for 2024, we asked each of the medical schools in the state to submit aggregate match data for these recent graduates, which they provided via email.
Findings
Class of 2019 Five Year Outcomes
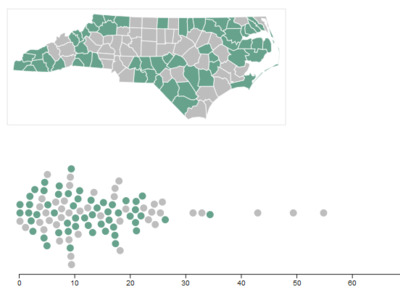
Figure 1 shows the number of 2019 North Carolina medical graduates in primary care.
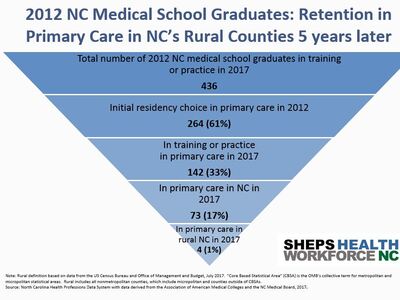
Figure 1. Retention of 2019 NC Medical Graduates in NC Rural Primary Care Five Years After Graduating
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. Rural source: US Census Bureau, Office of Management and Budget, July 2023 and USDA Economic Research Service RUCA codes, 2010. Core based statistical area (CBSA) is the OMB’s collective term for metropolitan and micropolitan statistical areas. Here, rural areas include counties in micropolitan statistical areas, counties outside of CBSAs, and census tracts with a RUCA code of 4 or greater.
Out of the 628 medical school graduates in 2019, 62 (10%) were in training or practice in primary care in NC in 2024 (Figure 1). This represents a decrease from previous years when between 12% and 17% of the most recent graduating cohorts (the classes of 2010-2018), were in training or practice in primary care in NC five years after graduating. Less than 1% (n=5) of the 2019 cohort was in primary care in a rural NC county. This also shows a decline relative to previous years when between 1% and 3% of NC medical school graduates were in practice in primary care in rural NC five years after graduating.
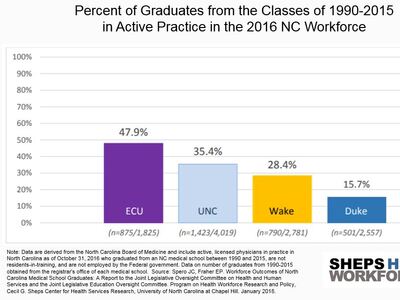
A greater percentage of graduates from the state’s public medical schools are retained in NC five years after graduating, compared to the state’s private medical schools (Figure 2). For the class of 2019, 46% of UNC graduates and 38% of ECU graduates were practicing in state in 2024. UNC has displayed a steady increase in in-state retention since the 2017 cohort.
Figure 2. Percent of NC Medical School Graduates in Training or Practice in North Carolina Five Years After Graduating
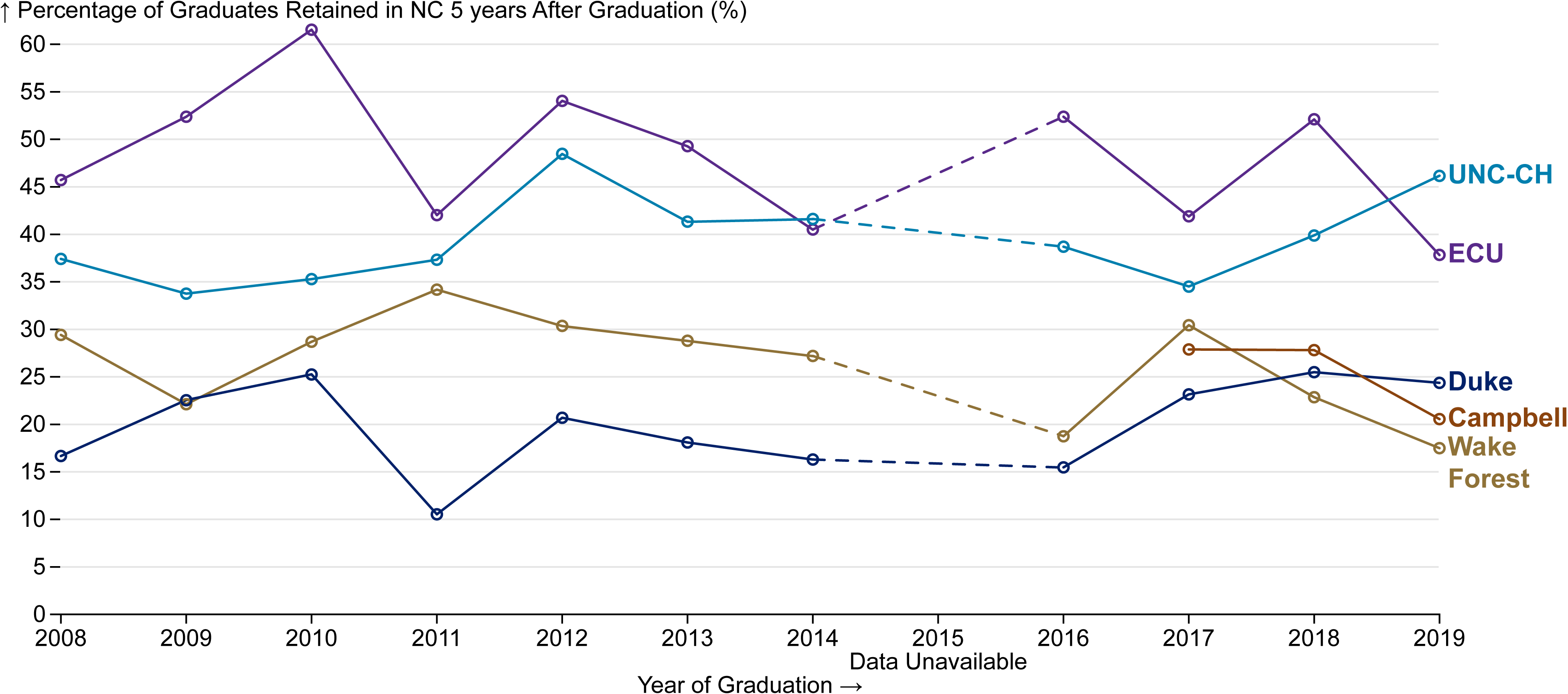
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC.
Figure 3 shows the primary care practice or training outcomes for each school’s 2019 graduates. Each individual figure is a version of Figure 1 for each school’s graduates. Very few graduates from any school are practicing primary care in a rural area, though Campbell had about 2% of their 2019 graduates practicing primary care in a rural area in North Carolina in 2024. UNC and ECU both retained at least 15% of their 2019 graduating classes in North Carolina practicing or training in primary care.
Figure 3. Physician Workforce Outcomes Five Years after Graduation, 2019 Medical School Graduates by School
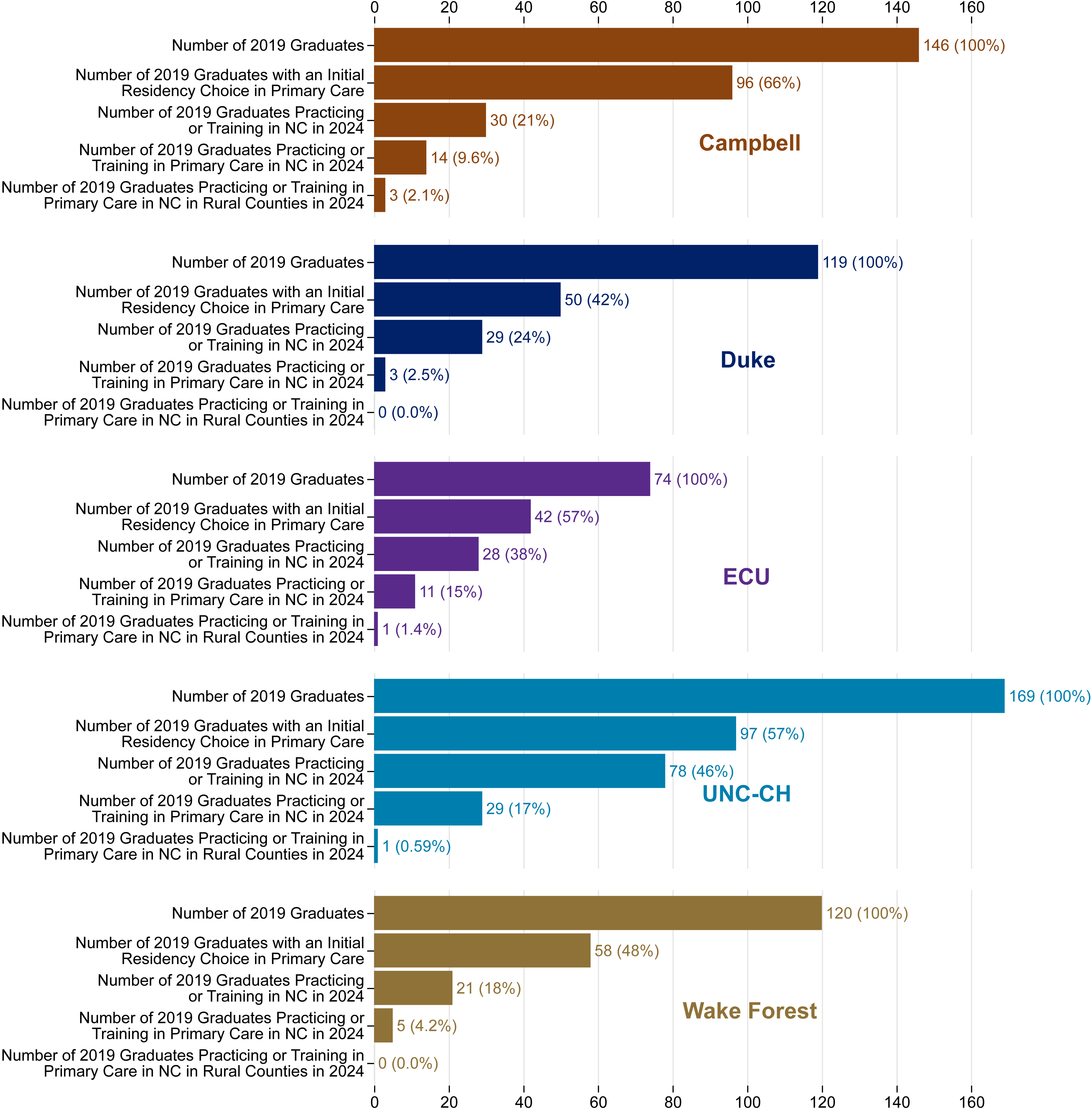
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. Rural source: US Census Bureau, Office of Management and Budget, July 2023 and USDA Economic Research Service RUCA codes, 2010. Core based statistical area (CBSA) is the OMB’s collective term for metropolitan and micropolitan statistical areas. Here, rural areas include counties in micropolitan statistical areas, counties outside of CBSAs, and census tracts with a RUCA code of 4 or greater.
Practice in Safety Net Settings and Most Economically Distressed Neighborhoods
Safety net providers are defined as health care facilities that provide a significant amount of health care and other health-related services to uninsured, Medicaid, and other vulnerable populations. Four graduates from the class of 2019 were in practice in safety net settings in NC in 2024, including two UNC graduates, one ECU graduate, and one Campbell graduate.
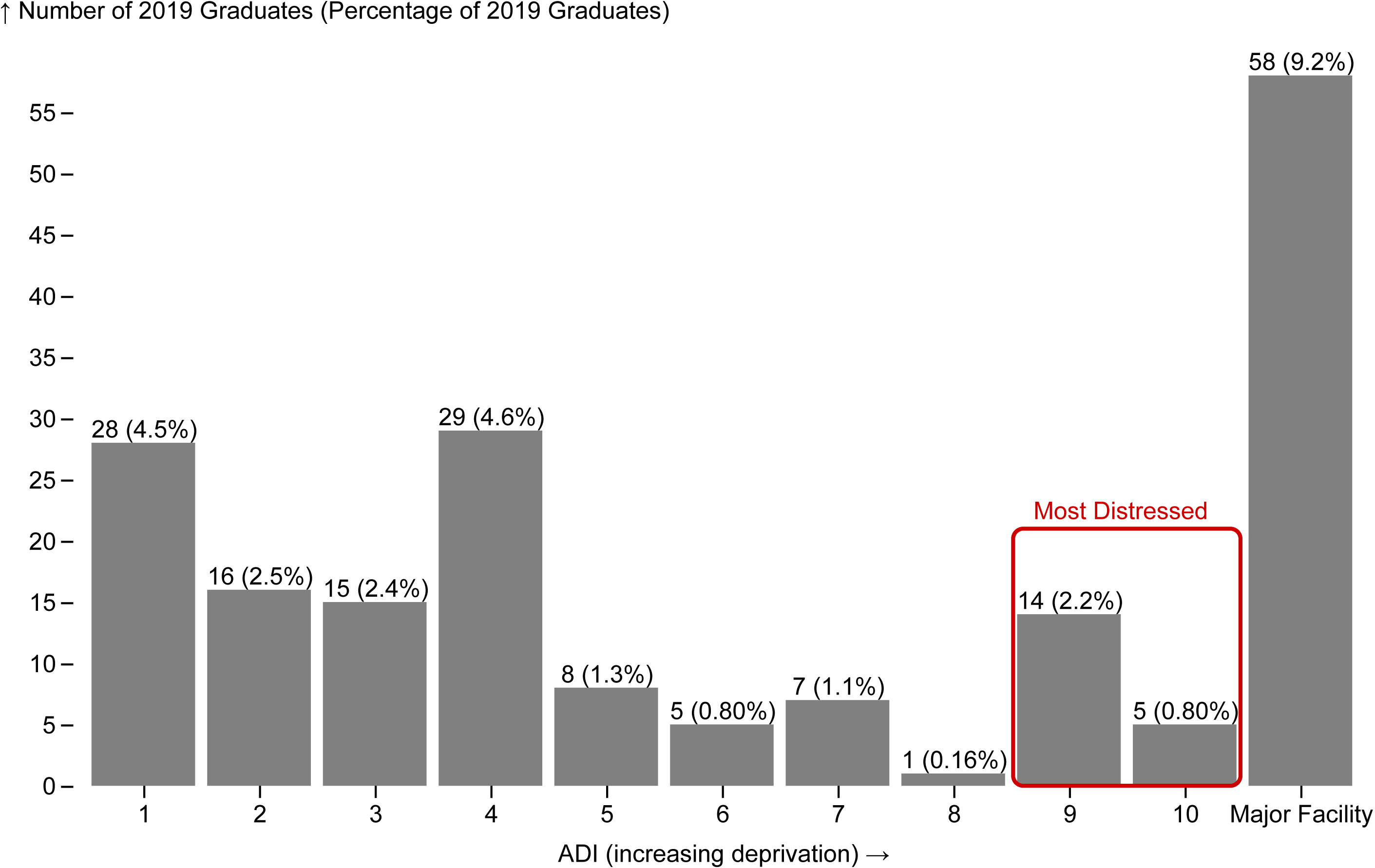
Figure 4 compares the Area Deprivation Index (ADI) of the neighborhoods where physicians who were retained in North Carolina five years after graduation report their primary practice location. Low scores indicate low levels of economic distress, and high scores indicate high levels of economic distress. Three percent (19/628) of the class of 2019 worked in a practice located in the most economically distressed neighborhoods (top quintile: ADI 9 and 10) five years after graduation.
ADI scores are not assigned for census block groups that are dominated by large facilities such as hospitals because they have so few people living these areas. ADI scores were not available for almost a third (31%, n=58/186) of the graduating class of 2019 who were still in North Carolina because their primary practice location was a large facility, most likely a hospital, which makes sense as many of these physicians are likely still in training.
Figures 4, 5, and 6 display only individuals who were licensed in North Carolina in 2024. While North Carolina graduates may be practicing in distressed areas or in needed areas of practice in other states, this report specifically focuses on service within North Carolina. Consequently, the 442 graduates (70% of the total class) who were practicing or training in another state, or who were not licensed in NC in 2024, are excluded from these charts. However, the percentages shown in the figures represent each group’s proportion of the total 2019 graduating class of 628 students, not just those who remained in North Carolina. As a result, the percentages across all categories total only 30% rather than 100%.
Figure 4. Neighborhood Disadvantage Status in 2024 of Physicians Retained in North Carolina Who Graduated from a NC Medical School in 2019
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. ADI Score obtained from the University of Wisconsin School of Medicine Public Health. 2022 Area Deprivation Index v4.0.1 Downloaded from https://www.neighborhoodatlas.medicine.wisc.edu/ on February 27, 2025.
Retention in Primary Care and Psychiatry Areas of Practice
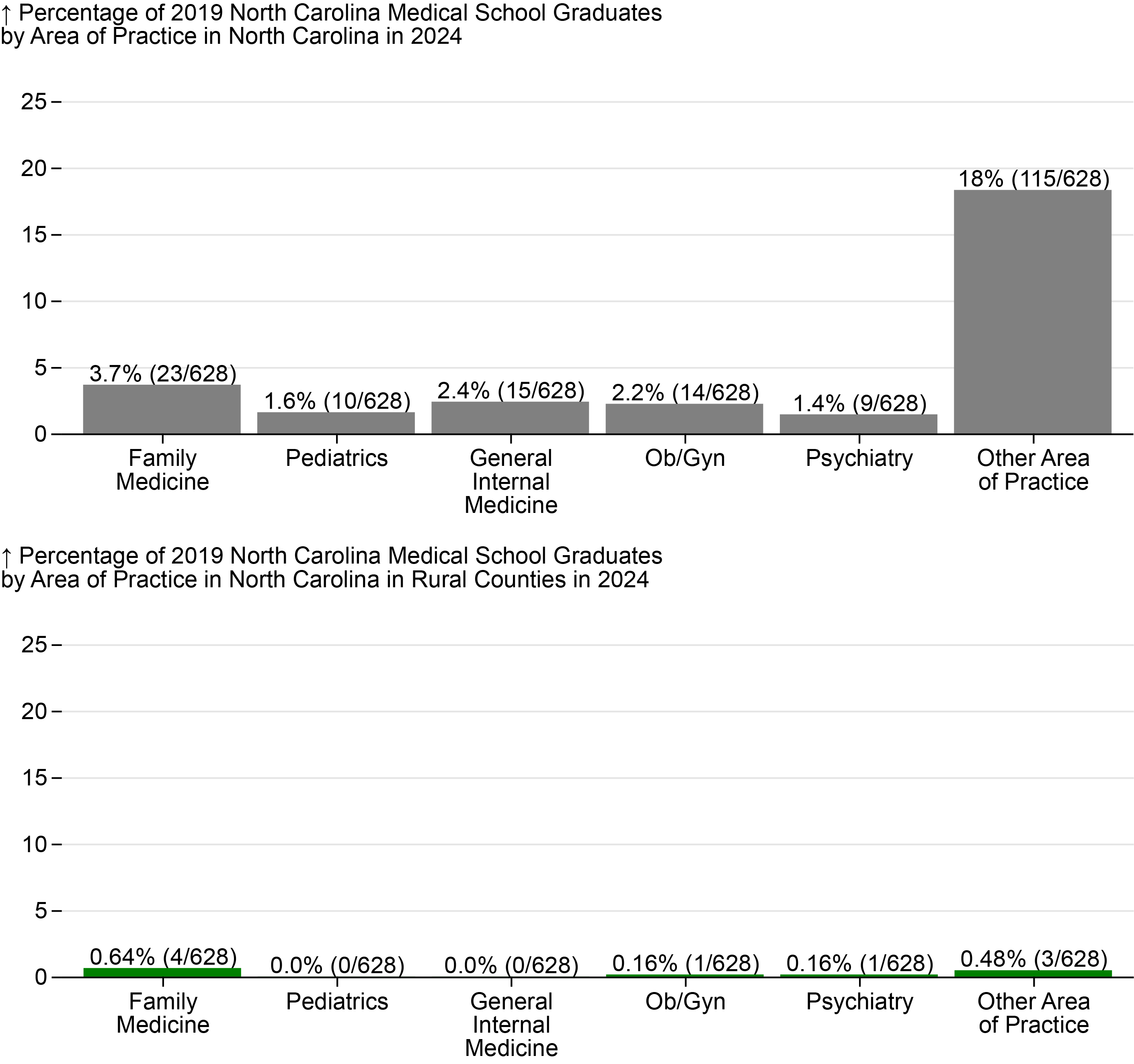
Figure 5 displays the outcomes for 2019 graduates by area of practice. Physicians report a primary area of practice to the NCMB each year of licensure. A physician’s primary area of practice can differ from their training specialty. The category “Other Area of Practice” includes all other specialties, including, for example, dermatology, hospitalist, and ophthalmology.
Figure 5. Percentage of 2019 Medical School Graduates Practicing or Training in Primary Care in North Carolina by Area of Practice in 2024, North Carolina Overall and Rural
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. Rural source: US Census Bureau, Office of Management and Budget, July 2023 and USDA Economic Research Service RUCA codes, 2010. Core based statistical area (CBSA) is the OMB’s collective term for metropolitan and micropolitan statistical areas. Here, rural areas include counties in micropolitan statistical areas, counties outside of CBSAs, and census tracts with a RUCA code of 4 or greater.
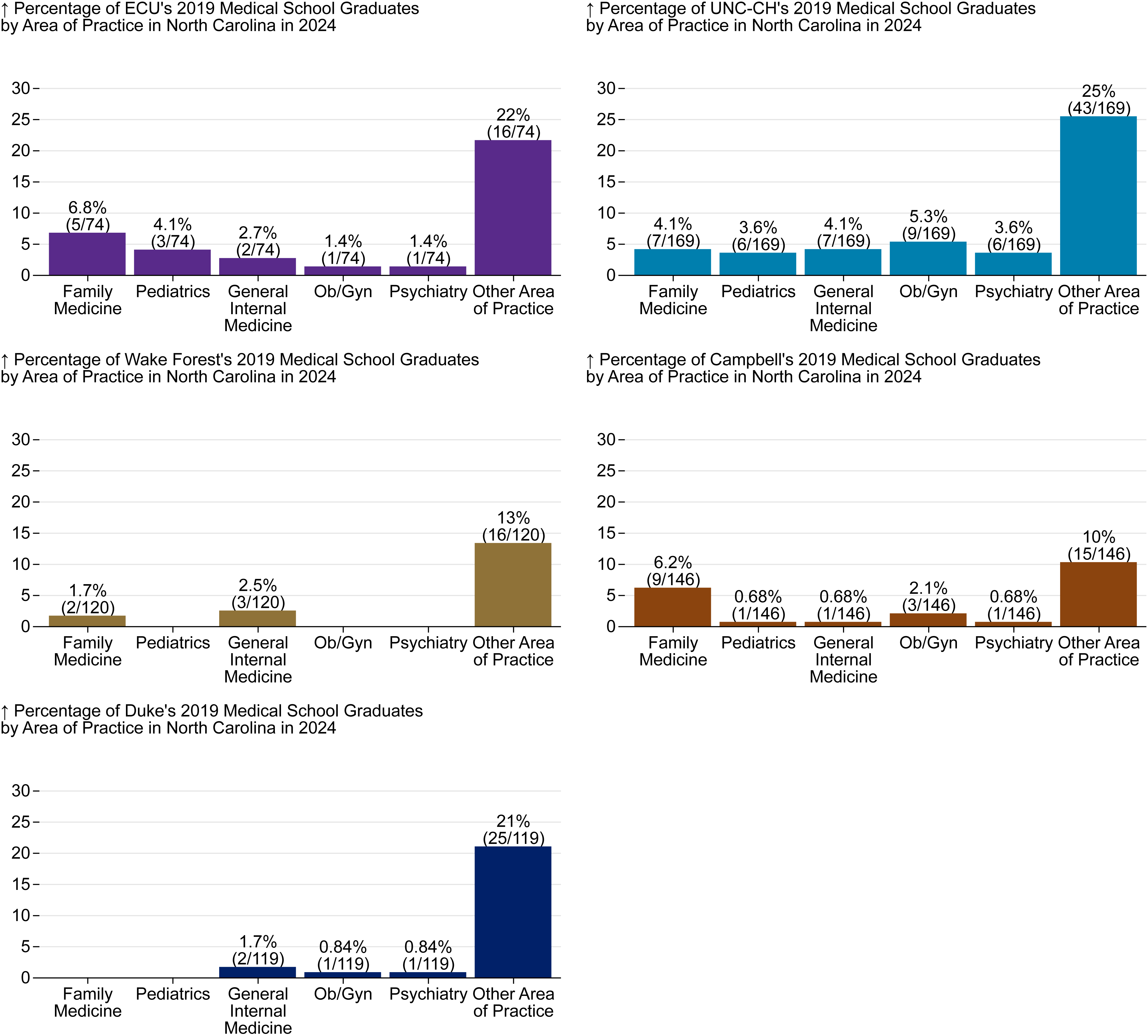
Figure 6 shows the same set of practice outcomes but for each school individually.
Figure 6. Percentage of 2019 Medical School Graduates Practicing or Training in Primary Care in North Carolina by Medical School and Area of Practice in 2024
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. Rural source: US Census Bureau, Office of Management and Budget, July 2023 and USDA Economic Research Service RUCA codes, 2010. Core based statistical area (CBSA) is the OMB’s collective term for metropolitan and micropolitan statistical areas. Here, rural areas include counties in micropolitan statistical areas, counties outside of CBSAs, and census tracts with a RUCA code of 4 or greater.
Class of 2014 Five Year Outcomes
We also tracked 2014 graduates of NC medical schools to determine where graduates were ten years following graduation from medical school. As noted previously, ten years post-graduation from medical school allows time for physicians to complete residency and fellowship training and settle into practice. A higher percentage of graduates are in primary care practice in rural areas ten years after graduation compared to five years after. This may indicate that some NC graduates do a residency out-of-state and then return to practice in NC or that some of the efforts currently underway to encourage medical students to practice in NC take a while to take effect but perhaps are starting to do so.
Figure 7 illustrates the aggregate outcome of North Carolina’s medical school graduates ten years after graduation in 2014. The total number of graduates in 2014 is much lower than in 2019, because Campbell had not yet graduated its first class.
Figure 7. Retention of 2014 NC Medical Graduates in NC Rural Primary Care Five Years After Graduating
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. Rural source: US Census Bureau, Office of Management and Budget, July 2023 and USDA Economic Research Service RUCA codes, 2010. Core based statistical area (CBSA) is the OMB’s collective term for metropolitan and micropolitan statistical areas. Here, rural areas include counties in micropolitan statistical areas, counties outside of CBSAs, and census tracts with a RUCA code of 4 or greater.
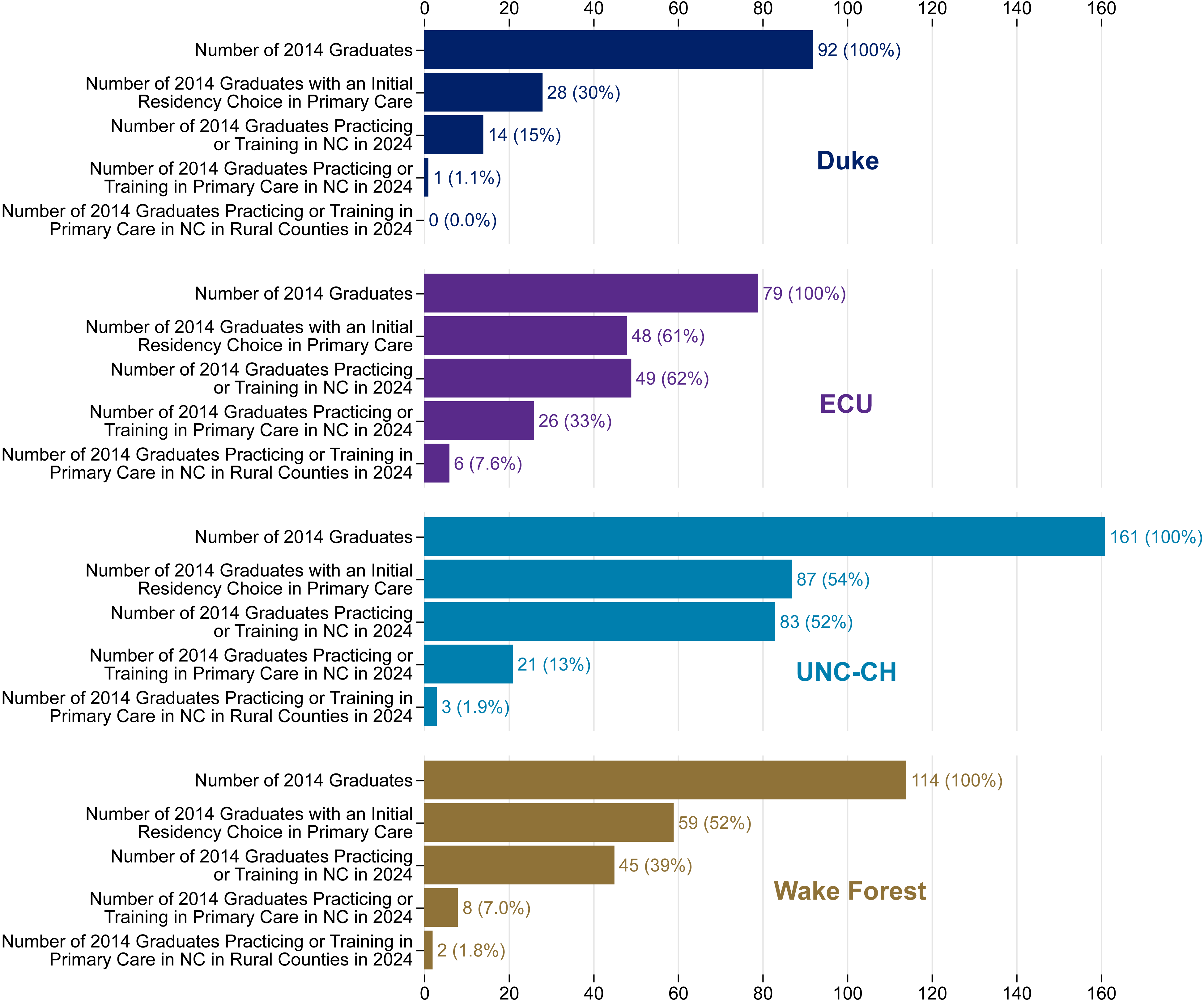
The retention of primary care providers for each school’s 2014 graduates is illustrated in Figure 8. One third (n = 26) of 2014 ECU graduates were practicing primary care in North Carolina in 2024.
Figure 8. Physician Workforce Outcomes Five Years after Graduation, 2014 Medical School Graduates by School
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. Rural source: US Census Bureau, Office of Management and Budget, July 2023 and USDA Economic Research Service RUCA codes, 2010. Core based statistical area (CBSA) is the OMB’s collective term for metropolitan and micropolitan statistical areas. Here, rural areas include counties in micropolitan statistical areas, counties outside of CBSAs, and census tracts with a RUCA code of 4 or greater.
Practice in Safety Net Settings and Most Economically Distressed Neighborhoods
Nine graduates from the class of 2014 were in practice in safety net settings in North Carolina in 2024, including five UNC graduates, three Wake Forest graduates, and one ECU graduate. This was a greater number than the 2019 cohort. While it would be hard to draw conclusions from these small numbers, it is possible that individuals are still in training at five years, which would typically be at a larger medical center, instead of a safety net setting.
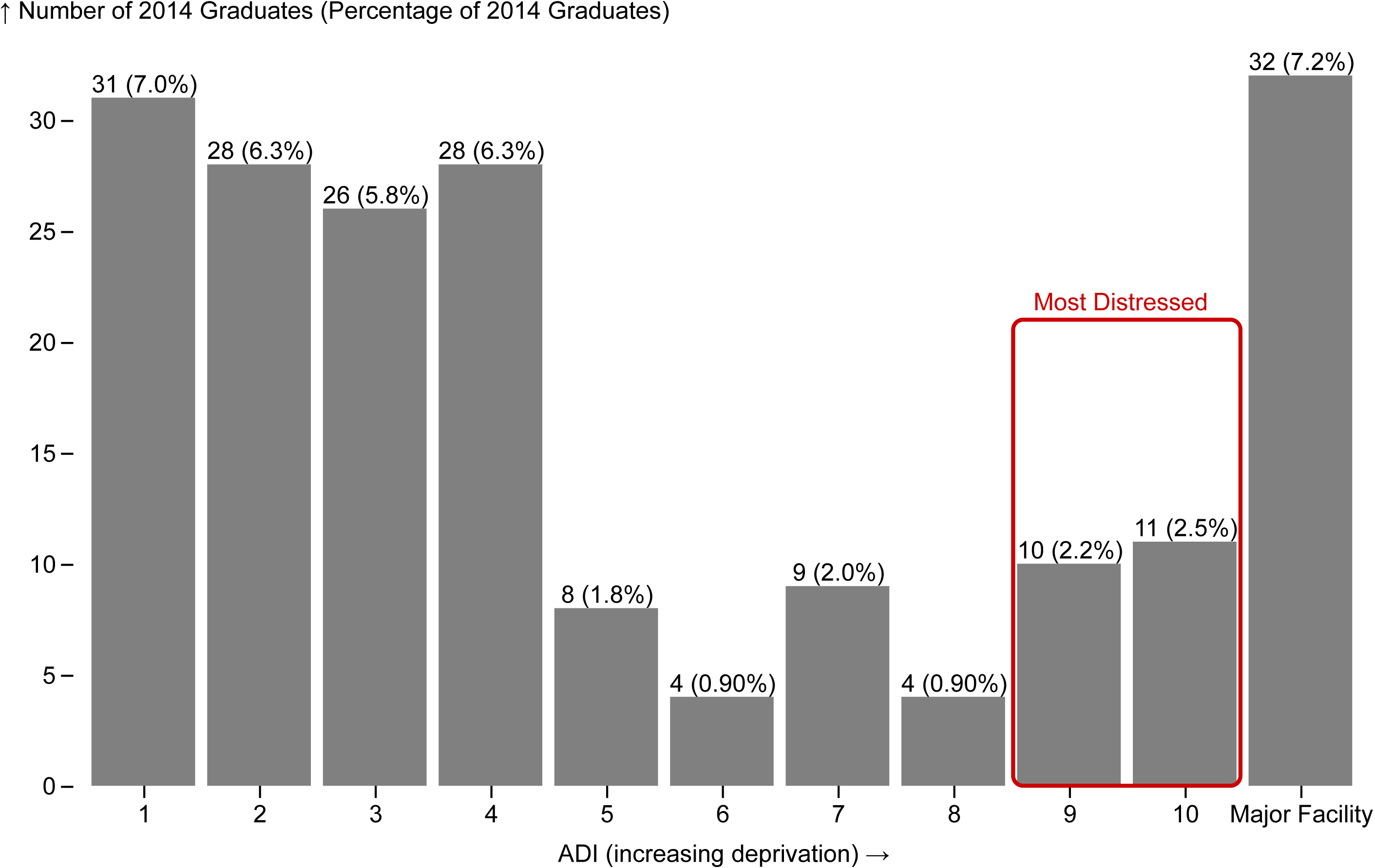
Figure 9 compares the Area Deprivation Index (ADI) of the neighborhoods in North Carolina where physicians from the class of 2014 report their primary practice location in 2024. Almost five percent (n=21/446) of the class of 2014 worked in a practice location in the most economically distressed neighborhoods (top quintile) ten years after graduation. As with the 2019 cohort, note the large proportion of graduates for whom an ADI score is not available because their practice location is a major facility. Of course, depending on the location and type of facility, many of these graduates will also be serving many economically distressed patients.
Figures 9, 10, and 11 display only individuals who were licensed in North Carolina in 2024. While graduates from this cohort may be practicing in distressed areas or in needed areas of practice in other states, this report specifically focuses on service within North Carolina. Consequently, the 255 graduates (57% of the total class) who were practicing or training in another state, or who were not licensed in NC in 2024, are excluded from these charts. However, the percentages shown in the figures represent each group’s proportion of the total graduating class of 446 students, not just those who remained in North Carolina. As a result, the percentages across all categories total only 43% , rather than 100%.
Figure 9. Neighborhood Disadvantage Status in 2024 of Physicians Retained in North Carolina Who Graduated from a NC Medical School in 2014
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. ADI Score obtained from the University of Wisconsin School of Medicine Public Health. 2022 Area Deprivation Index v4.0.1 Downloaded from https://www.neighborhoodatlas.medicine.wisc.edu/ on February 27, 2025.
Practice in Safety Net Settings and Most Economically Distressed Neighborhoods
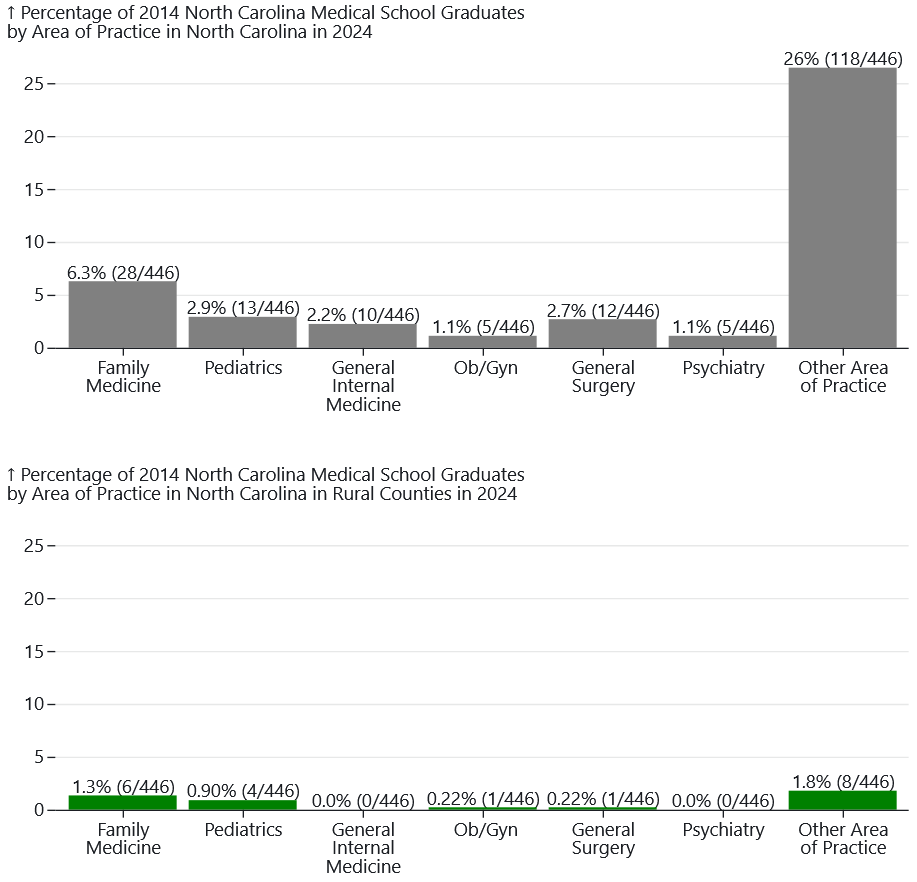
Figure 10 shows outcomes for 2014 graduates who are in North Carolina and have a primary care area of practice, or who are practicing psychiatry or general surgery. The outcomes for general surgery are reported here for the 2014 cohort, but not for the 2019 cohort, because general surgery residencies typically last five years, and many general surgeons complete a subspecialty fellowship afterwards. For this reason, reporting on general surgery practice outcomes at five-years post-graduation may be misleading.
Figure 10. Percentage of 2014 Medical School Graduates Practicing or Training in Primary Care in North Carolina by Area of Practice in 2024, North Carolina Overall and Rural
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. Rural source: US Census Bureau, Office of Management and Budget, July 2023 and USDA Economic Research Service RUCA codes, 2010. Core based statistical area (CBSA) is the OMB’s collective term for metropolitan and micropolitan statistical areas. Here, rural areas include counties in micropolitan statistical areas, counties outside of CBSAs, and census tracts with a RUCA code of 4 or greater.
Figure 11 shows the same area of practice outcomes, but for each school individually.
Figure 11. Percentage of 2019 Medical School Graduates Practicing or Training in Primary Care in North Carolina by Medical School and Area of Practice in 2024
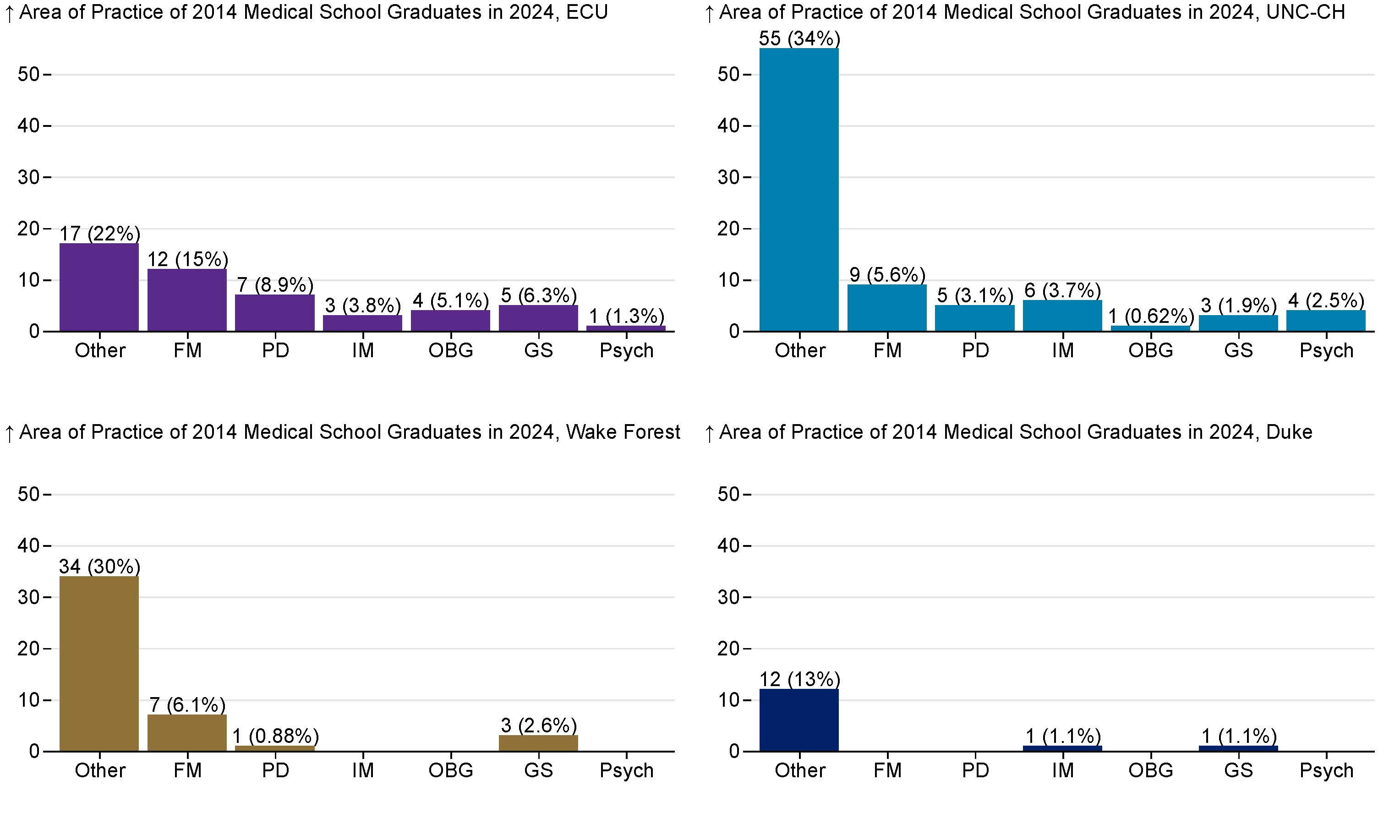
Family Medicine (FM), Pediatrics (PD), General Internal Medicine (IM), Ob/Gyn(OBG), Psychiatry (Pysch), Other. Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: North Carolina Health Professions Data System with data derived from the NC Medical Board and the AAMC, 2024. Rural source: US Census Bureau, Office of Management and Budget, July 2023 and USDA Economic Research Service RUCA codes, 2010. Core based statistical area (CBSA) is the OMB’s collective term for metropolitan and micropolitan statistical areas. Here, rural areas include counties in micropolitan statistical areas, counties outside of CBSAs, and census tracts with a RUCA code of 4 or greater.
Initial Match Data: 2024 Graduating Cohort
As mentioned earlier, this report does not emphasize initial match data from the NC medical schools. Residents sometimes switch specialties or residency programs throughout the course of their training, and many subspecialize. Initial matches to “primary care” specialties (Family Medicine, Internal Medicine, Pediatrics, Internal Medicine-Pediatrics, and Obstetrics & Gynecology) are inflated compared to the number of graduates eventually expected to practice in those fields. We also track two other needed specialties in NC: psychiatry and general surgery. Prior trends indicate that many NC graduates, including most of those who match to Internal Medicine and General Surgery, will go on to complete fellowship training and eventually practice in a sub-specialty field. For instance, 126 graduates from 2014 entered a general internal medicine residency program, but 83% subsequently pursued subspecialty training (not including geriatric medicine). Family Medicine is an exception to this trend.
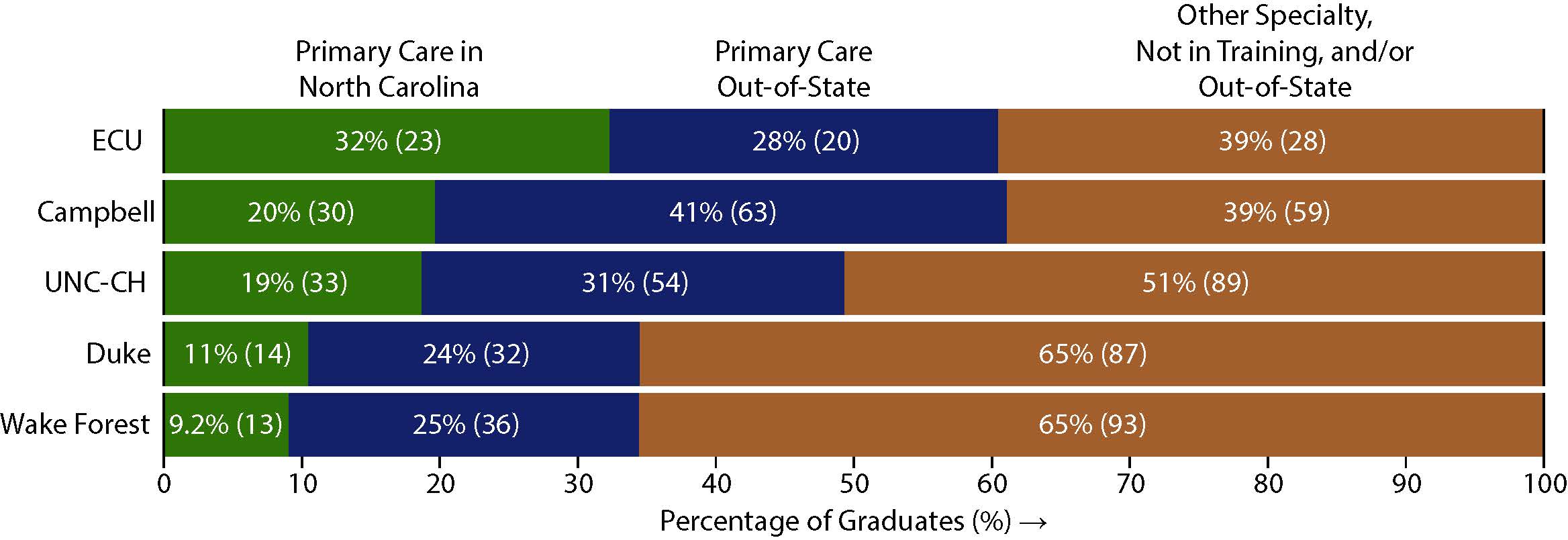
Figure 12 shows the proportion of each school’s 2024 graduates who had an initial match to a primary care residency in North Carolina or in another state. Across the five schools 318 of 674 graduates (47%) were initially matched into primary care with 113 (17%) matching into primary care in North Carolina. ECU matched the greatest proportion to primary care residencies in North Carolina (32%, n = 23). However, Campbell and ECU both matched about 61% of their graduates to primary care residencies, including both in-state and out-of-state matches.
Figure 12. Initial Matches of 2024 Graduates to Primary Care Residencies by School
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: the respective medical schools, 2024.
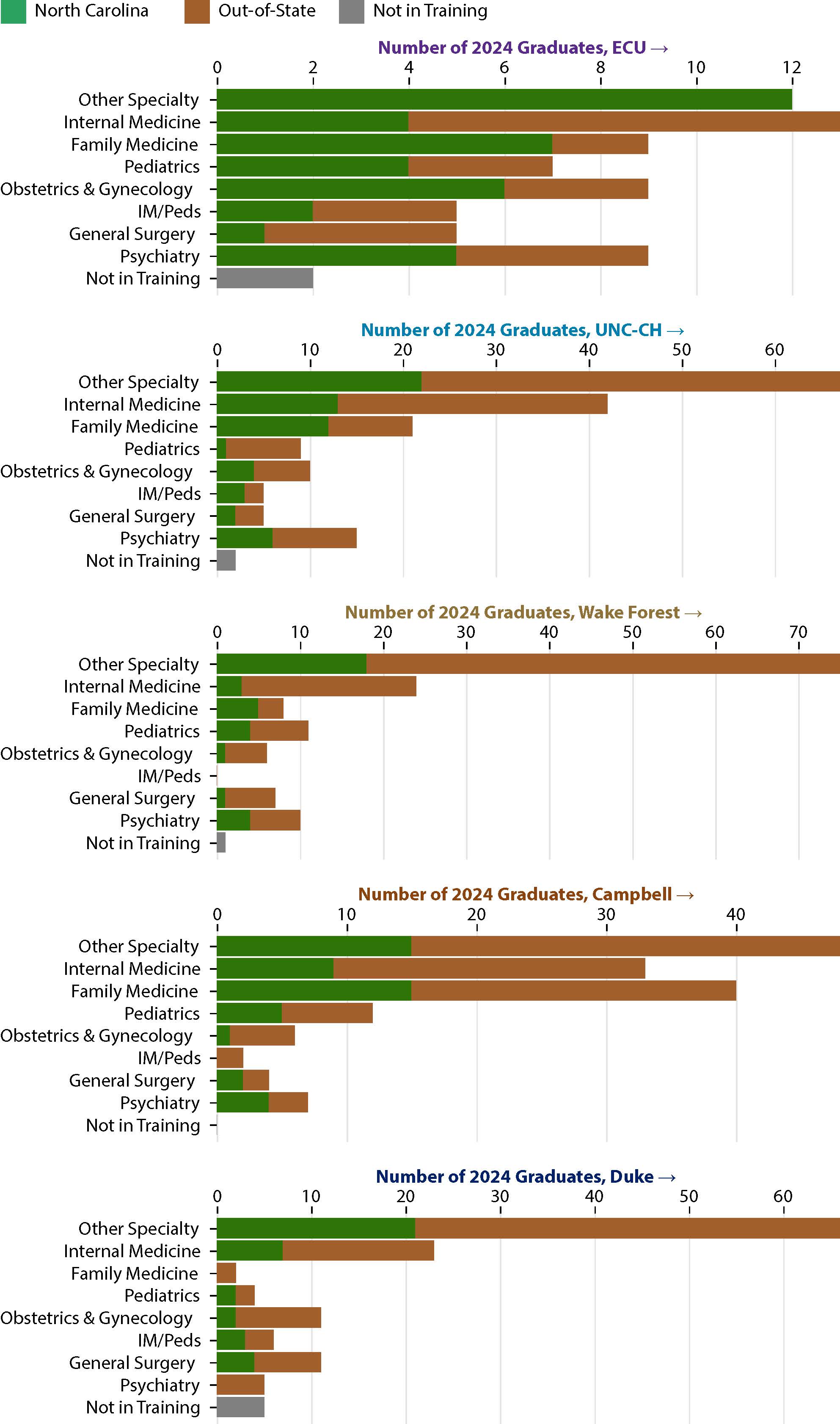
Figure 13 displays the number of 2024 graduates who matched to primary care specialties, general surgery, or psychiatry. (Note that the axes are scaled to each school’s number of graduates.) ECU and Campbell led on Family Medicine residency matches, with 10% of ECU’s graduating class matching to a Family Medicine residency in North Carolina, and more than a quarter of Campbell graduates matching to a Family Medicine residency anywhere. UNC matched the greatest number (13) and percentage (7.4%) of graduates to Internal Medicine residencies in NC.
Figure 13. Number of 2024 Graduates by School and Initial Match Specialty, Selected
Produced by the Program on Health Workforce Research and Policy, Sheps Center for Health Services Research, University of North Carolina at Chapel Hill. Source: the respective medical schools, 2024.
Discussion
In summary, out of the 628 medical school graduates from North Carolina’s five medical schools in 2019, 10% were in training or practice in primary care in NC in 2024 and less than 1% were in primary care in a rural county five years after graduation. Both the percent of medical graduates practicing in primary care and in rural areas is lower than in previous years. A greater percentage of graduates from the state’s public medical schools are retained in NC five years after graduating, compared to the state’s private medical schools. Four graduates practiced in safety net settings and 3% of the class of 2019 worked in practices located in the most economically distressed neighborhoods in North Carolina.
By comparison, tracking outcomes ten years after graduation revealed that a higher percentage of graduates from 2014 were in in primary care practice (13%) and in primary care practice in rural areas (2.5%) ten years after graduation than five years after graduation. Nine graduates from the class of 2014 were in practice in safety net settings in North Carolina in 2024, which is also a greater number of graduates than the 2019 cohort. Almost 5% of the class of 2014 worked in a practice location in the most economically distressed neighborhoods, as measured by the ADI score, ten years after graduation. The outcomes for general surgery are reported for the 2014 cohort, but not for the 2019 cohort, because general surgery residencies typically last five years, and many general surgeons complete a sub-specialty fellowship afterwards. North Carolina retained 2.7% of graduates (12/446 graduates) in general surgery practice ten years after graduation and 0.22% (1/446 graduates) in general surgery in a rural county ten years after graduation from medical school.
These data show that retention rates for NC medical school graduates in primary care areas after graduation from a NC medical school remain low. By comparing 5-year and 10-year post graduation retention rates, we see that a higher percentage of graduates is retained in primary care, rural, safety net and disadvantaged practice areas 10-years after graduating from a NC medical school. This may indicate that NC medical school graduates are leaving the state for residency training but then returning after pursuing residency training out of state or that some previously implemented interventions are beginning to have effect.4, 5
Appendix A
Self-reported responses to requests for information about what each North Carolina medical school is doing to try to increase the number of students who will practice primary care in rural North Carolina.
Campbell University School of Osteopathic Medicine
The mission of the Campbell University School of Osteopathic Medicine (CUSOM) is to educate and prepare community–based osteopathic physicians in a Christian environment to care for the rural and underserved populations in North Carolina, the Southeastern United States, and the nation. The focus on community-based care is significant as it recognizes the unique health care needs of rural and underserved populations. The preparation to enter those environments is unique and has been a core focus for our school. The Christian environment that we foster has played a significant role in shaping the values and beliefs of our graduates and shaping the way they approach their work as physicians. By instilling a strong sense of compassion, empathy, and ethical principles in its graduates, CUSOM is helping to ensure that they are well-prepared to provide high-quality, patient-centered care that is consistent with institutional values.
Campbell University School of Medicine opened its doors to its inaugural class of 162 students in 2013. Campbell University also became the first College of Osteopathic Medicine to serve as an ACGME sponsoring institution for Graduate Medical Education. As a sponsoring institution, Campbell University has provided support and resources to its affiliated residency programs ensuring that they meet the standards and requirements set forth by the ACGME. 15 osteopathic programs successfully transitioned to ACGME accreditation under Campbell University’s Sponsoring Institution. Campbell University now serves as the Sponsor for 12 ACGME-accredited programs in partnership with 4 hospitals and systems. We serve as an educational affiliate partner for 3 additional hospital systems in NC.
Medical Student Impacts
The graduating class of 2017 (our inaugural class) would have completed 3-year residencies in 2020, 4-year residencies in 2021, and 5-year residency programs in 2022.
The graduating class of 2018 would have completed 3-year residencies in 2021, 4-year residencies in 2022, and 5-year residency programs in 2023.
The graduating class of 2019 would have finished their 5-year residencies in 2024.
A total of 189 CUSOM graduates entered the workforce in 2024, where 41 graduates stayed in NC and 76 graduates stayed in the southeastern US. According to the data that we have on the first four classes and partial for 2019 and 2020, 410 of our graduates are currently in practice in southeastern US with 225 of those graduates (55%) located in the state of North Carolina. As of 2024, 66 Family Medicine CUSOM physicians are practicing in NC, and 109 are practicing in the southeastern US. 70 Internal Medicine CUSOM physicians are practicing in NC, and 112 are practicing in the southeastern US.
Overall, these trends suggest that CUSOM is making a positive contribution to the development of the physician workforce in North Carolina and that its graduates are wellprepared to enter the workforce and provide high-quality care to patients. The strong commitment to primary care fields and specific areas of need is critical to positively impacting our state’s ability to provide comprehensive, patient-centered care.
Graduate Medical Education Impacts
Campbell University had a goal of having a net neutral impact on the number of graduate medical education positions by creating enough positions that we would not graduate more medical students than the graduate medical education positions we created. To date, Campbell University has started 25 residency and fellowship programs in North and South Carolina. And as of 2024, we have transitioned to serving as an educational affiliate for the Cape Fear Valley and UNC Heath Southeastern programs while assisting both sites with becoming their own sponsoring institutions. Our current programs contain 124 GME positions in Family Medicine (x4), Internal Medicine, Dermatology, and Transitional Year (x3). We have fellowship programs in Sports Medicine (x2) and Micrographic Surgery.
Campbell University had our first resident start in 2014 as an educational partner through the AOA. Since that time, Campbell University Graduate Medical Education programs have placed 87 providers into active clinical practice with 32 of those remaining in North Carolina (38%) and 19/32 (59%) being in the fields of Family Medicine or Internal Medicine. Primary care is a critical component of health care, as it provides the foundation for patient care and helps to manage the overall health and well-being of individuals and populations. A solid primary care workforce is essential to ensuring that patients have access to comprehensive, high-quality care and that health care systems can effectively address the health needs of their communities.
Summary
Campbell University Graduates are now currently active in 47 of North Carolina’s 100 counties. The full impact of Campbell University graduates to the physician workforce is still emerging. 2020 saw the inaugural class graduate from 3-year primary care programs. 2022 saw the first graduates in Surgery and Psychiatry from Campbell University GME programs. Combining the efforts of our medical school and our graduate medical education programs, Campbell University has placed 189 new providers in 47 North Carolina counties as of April 2025. Additionally, 30 of the 47 occupied North Carolina counties are underserved, which displays that Campbell University is meeting its mission of producing graduates to work in rural and underserved counties.
Duke University School of Medicine
Duke provides medical student clinical rotations. The goals of this program are for students to learn clinical skills in the context of a local community and to appreciate the effects of culture and context on health and health behaviors. Duke students may rotate through clinics in Person and Durham County health departments evaluating and following patients in these rural communities.
Duke also offers the Primary Care Leadership Track (PCLT), the goal of which is to create change agents for the system through primary care and leaders in the health care profession. The 4- year program offers leadership training, a longitudinal-integrated 2nd year clerkship, which includes following pregnant mothers and delivering their babies, time for service with a community agency, and 3rd year research in community-engaged population health. PCLT graduates have chosen primary care residencies: family medicine (outpatient adults, children, and prenatal care), general internal medicine (adults only), primary care pediatrics (children only), pediatrics/psychiatry, medicine/psychiatry, family medicine/psychiatry and Obstetrics/gynecology.
Through our MS1 reflection exercises and lunch discussions, specialty handbook, and specialty advisor community, the Career Exploration and Career Destination program helps our students identify the values and skills that will be most meaningful to them in clinical practice and match that with the correct specialty, including those rooted in the delivery of primary care.
Duke offers a primary care student interest group open to all students that has career panels 1-2 times a year and meets regularly.
ECU Brody School of Medicine
The Brody School of Medicine (BSOM) stands apart with its three-part mission to increase the supply of primary care physicians serving the state, improve the health and well-being of the region, and train physicians who will meet the state’s health care needs. This distinctive mission makes BSOM a top choice for those intending to practice primary care specialties in our state.
Residency Match and Future Practice
The success of our students is a testament to the quality of education at BSOM. BSOM has graduated about 400 students in the last five years, and 65% of those with medical residencies in North Carolina practice in primary care specialties. We continue to see this pattern in our recent Class of 2025, where 53% of our graduates match in primary care and 43% of them in North Carolina. As a result, BSOM continues to be ranked above the 90th percentile in the percentage of graduates practicing primary care and in-state, as well as in the Top 25 medical schools with the most graduates practicing in Health Professional Shortage Areas (HPSAs).
Medical Curriculum
Match outcomes reflect our medical curriculum. Starting in the foundational years of the curriculum, BSOM medical students are expected to participate in and complete primary care activities at community sites throughout the medical curriculum.
During the second year, students have scheduled preceptorship dates every fall when they shadow and work with physicians and health professionals at practices in North Carolina (only in-state practices are approved). As students progress in the medical curriculum, our Family Medicine, Internal Medicine, and Pediatrics clerkships have allocated two to four weeks in their schedules for students to spend their time practicing with affiliated faculty at community sites locally and across the state, mostly in ambulatory clinics. Additionally, students can choose from over 170 electives in the third and fourth year of the medical curriculum, of which more than half of these experiences are in primary care specialties. These elective courses give our students additional opportunities to interact with other professionals and community resources, mainly in North Carolina and the Eastern region of our state, in providing comprehensive and continuing care, and working with different types of care given in other settings and populations outside the university medical center.
These experiences have made BSOM graduates confident that they have acquired the technical skills needed to begin a residency program, feel prepared to care for patients from different backgrounds, and have the communication skills necessary to interact with patients and health professionals. As a result, over 95% of BSOM graduates in primary care residencies are rated as meeting or exceeding expectations in their first year of the residency program.
Service and Research
In addition to curricular and learning measures focusing on primary care and early immersion in patient care experiences, non-curricular events and programs have been created for students to interact with primary care practitioners.
BSOM Distinction Track Program allows medical students to pursue independently an area of interest in their medical career. The program has five tracks aligned with our missions: health system transformation and leadership, medical education and teaching, research, service learning, and medical humanities and ethics. While in the program, medical students work with faculty mentors on a longitudinal project that culminates as a capstone in the fourth year of the curriculum. Many projects are in primary care specialties, with primary care clinicians, in topics that relate to our population in eastern North Carolina, and improvements to the health and wellbeing of our region. The following are examples of past and in-progress projects for some of the tracks:
- Reducing Musculoskeletal Injury Among Agricultural Workers
- Substance Use Amongst Youth in Pitt County
- Improving Education Disparities Experienced by Homeless Youth in Eastern North Carolina
- Assessing the Use of Retinal Imaging in Detection of Hypertension and/or Diabetes in North Carolina Farmworkers
- Medical Education Factors Impact to Practice Rural Medicine
- Decreasing Outpatient Times for Pediatric Specialty Care Clinic Visits, Closing the Gap between Primary and Specialty care – A Crucial Intervention to Boost Vaccination Rates for Cystic Fibrosis patients at ECU Health
- Improving Care for People with Diabetes in the ECU Adult and Pediatric Healthcare Clinic. The medical students volunteer at various free clinics in our region, primarily the Pitt County Care Clinic. By graduation, over 80% of BSOM graduates have experience with a free clinic for the underserved population, expertise related to health disparities, and have learned the proper use of an interpreter when needed.
The combination of our medical curriculum, non-curricular experiences, and our students’ desire to pursue primary care specialties and practice in underserved and underrepresented populations is why BSOM continues to be ranked nationally in the 92nd percentile of graduates practicing in rural areas and the 94th percentile of graduates practicing in primary care.
University of North Carolina at Chapel Hill School of Medicine
Our mission is to improve the health and wellbeing of North Carolinians and others whom we serve through excellence in patient care, education, and research. We have several programs that have historically supported those interested in primary care, and we have also developed an innovative program that combined our historic programs to provide even greater opportunities for our students to explore and experience rural and primary care. This merger allowed for an alignment of resources and an expansion of learning opportunities for students.
Kenan Rural Primary Care Scholars Program – With support of the Sarah Graham Kenan Endowment and the William R. Kenan, Jr. Charitable Trust, the Kenan Primary Care Scholars Program offered UND medical students rural experiences in central, eastern, and western North Carolina. These longitudinal exposures during medical school prepare students for careers in rural primary care while also providing financial support and enrichment experiences to sustain their commitment to rural primary care in NC.
This program started in 2013 and expanded in 2017 from one cohort to three cohorts. Here are the results of this program thus far:
- Through 2024, there have been 57 graduates of which 49 (85%) matched into primary care residencies including combined medicine-pediatrics programs.
- Among the 49, 31 (63%) matched in NC residency programs.
- Of the 24 who have completed primary care residencies, 14 (59%) are practicing in NC and 1 that will begin practice in NC in 2025 following residency completion. Two (2) additional scholars practiced in NC for 2 years prior to leaving for family reasons (total 17 of the 24 or 71% have served NC).
- 11 of the 17 practiced, or are currently practicing (including the 2025 graduate), in a rural NC county (65%).
- 7 of the 24 who have completed residency are currently practicing out of state with stated plans to return to NC in the future. One is in VA serving rural border NC county patients.
FIRST (Fully Integrated Readiness for Service Training) Program – The FIRST Program began in 2016 with 3 matriculants in the field of Family Medicine and was further expanded to various primary care specialties and GME programs in 2019 via an American Medical Association (AMA) Reimaging Residency Grant. The FIRST Program operates as a three-year accelerated program with a mission to increase the number of students seeking rural and underserved primary care residency placements and careers in NC. It consists of three parts: 1) An enhanced 3-year medical school curriculum, 2) A directed pathway into an affiliated residency program, and 3) Three years of service in a rural or underserved area of NC with ongoing support in practice. Students are recruited to the FIRST Program during their first year of medical school. The FIRST Program promotes close faculty mentorship and familiarity with healthcare systems, including early and longitudinal integration into clinical care, and fosters a close cohort of fellow students. The affiliated GME Programs FIRST students can participate in encompass six specialties: 1) Family Medicine, 2) General Surgery, 3) Internal Medicine, 4) Medicine-Pediatrics, 5) Pediatrics, and 6) Psychiatry with ties to residency programs through partnerships with Mountain Area Health Education Center (MAHEC), Southeastern Area Health Education Center (SEAHEC), Greensboro, WakeMed in Raleigh, and Novant Hospital in Charlotte.
To date (as of June 2024), the results of the FIRST Program are:
- 50 students have accepted into the FIRST Program
- Currently 7 total participants have graduated residency and are in practice. 100% of the graduates are practicing Family Medicine in medically underserved communities in North Carolina (e.g. Siler City, Clyde, Wilmington, and Pittsboro).
- There are currently 24 students currently in the UME portion of FIRST and 9 students in the GME portion, all in the state of NC.
- Of our 41 FIRST participants, we have 3 students committed to Internal Medicine, 1 student committed to Medicine-Pediatrics, 6 students committed to Pediatrics, 5 students committed to psychiatry, 1 student committed to Surgery, and 24 students committed to Family Medicine.
Community Health Training (CHT) Program – Beginning with the medical school class that matriculated in Fall 2024, the FIRST, Kenan Rural, and PROMISE Scholars programs have merged to form a unified pipeline: the Community Health Training (CHT) Program. This program builds upon the well-established curriculum and structure of the Kenan Rural Scholars and FIRST Programs, both of which have a strong track record of training physicians to serve North Carolina’s rural and underserved communities. The former PROMISE Scholars program further enhances CHT by providing additional scholarship support to students committed to this mission.
CHT represents a cohesive, mission-driven effort by the School of Medicine to recruit and train future physicians through a structured, curriculum-based program focused on community medicine. The program is dedicated to cultivating interest in primary care and rural medicine, ensuring that students are equipped to make a lasting impact in medically underserved areas across North Carolina.
The Community Health Training (CHT) Program is a two-pathway track designed to prepare students for community medicine in rural and medically underserved settings. CHT scholars are united by a shared commitment to improving healthcare access and quality for North Carolina’s most vulnerable populations by reducing health disparities and addressing physician shortages.
The mission of CHT is to cultivate future physicians dedicated to serving diverse communities across North Carolina, particularly in rural and medically underserved areas. To further this goal, CHT not only provides undergraduate medical training but also direct UME-to-GME pathways, ensuring a seamless transition from undergraduate medical education (UME) to graduate medical education (GME).
These pathways support students pursuing Psychiatry, General Surgery, Internal Medicine, Med-Peds, Family Medicine, and Pediatrics through partnerships with leading residency programs across North Carolina, including:
- Novant Health - Charlotte
- Novant Health - Wilmington
- WakeMed
- Cone Health
- Mountain Area Health Education Center (MAHEC)
- Asheville
- Hendersonville
- Boone
- UNC-Chapel Hill
By providing an accelerated 3-year community-focused UME to GME pathway and a flexible traditional 4-year pathway that allows students to explore GME programs, practice locations across North Carolina, and primary care specialties, CHT reinforces its commitment to training and retaining physicians in the state’s rural and underserved communities. This approach ensures that future healthcare leaders are well-prepared to address the unique needs of these populations while making informed decisions about their career trajectories
The inaugural cohort of CHT students were recruited from the UNC SOM class matriculating in 2024-2025, with 24 total Scholars were accepting into the CHT. Amongst the 24 students accepted, their career interests span the following breakdown:
Three-Year Pathway -
- Family Medicine (6 total students)
- Internal Medicine (3 total students)
- Pediatrics (2 total students)
- Med-Peds (1 student)
Four-Year Pathway - 12 total students
Through the Community Health Training Program (CHT) and direct UME-to-GME pathways, CHT is building a robust pipeline of future physicians dedicated to primary care, rural medicine, and improving health equity across North Carolina.
Important Pathway Programs before medical school – UNC SOM has a wide array of other programs that seek to connect high school and college students to rural primary care programs and interests. Examples include the Rural Health Summer Academy that offers rising high school seniors a week-long immersive experience on UNC’s SOM campus; the Rural Medicine Pathway Program, a partnership with the Carolina Covenant Scholars Program provides mentorship, guidance, and community engagement experiences to students from rural areas of North Carolina and helps prepare students to apply to UNC SOM.
Our SERVE portfolio of pathway programs continues to expand and elevate the work that began in the southeast part of the state in November 2022 through funding provided by Novant Health, UNC Health, and UNC School of Medicine; SERVE's outreach efforts are focused on reaching rural students in middle school, high school, and college in Bladen, Brunswick, Columbus, Pender, and New Hanover Counties, and it introduces students to healthcare workforce shortages in their counties, as well as across North Carolina. The programs have expanded to Chatham and Rockingham Counties, and have included students from Duplin, Johnston and Gaston counties as well over the last two years. SERVE programs also showcase multiple health professions careers and highlights the many paths students can take to get into those careers.
Moreover, SERVE has several additional pathway programs that have been created under its parent umbrella, including exploration events hosted in the above-listed communities like the On-Call Speaker Series, which connects providers who graduated from high schools in southeastern communities back to those schools to share their journeys with local students. SERVE also houses Health Career Exploration Events hosted with Cape Fear Community College in an effort to show students how they can start their healthcare journeys while in high school. The UNC Health Ingram Institutes’ SERVE pathways team has hosted over 150 students with Heal Day with the Heels, which brings high school and college students to UNC's campus for a day of learning about the path to medical school and other fields simulations, panels, and interaction with current medical students and faculty members. During the day, students work through a patient intake simulation, seeing professions interact as a care team and learning how different treatments are connected. The SERVE program can positively impact the North Carolina health professions workforce shortages by providing students early exposure to these careers and alerting them about the opportunities that lie in returning to their rural communities or other similar communities in North Carolina to practice. SERVE reached 4,741 students in 2024!
Wake Forest University School of Medicine
Wake Forest University School of Medicine (WFUSM) has been continuously accredited since prior to 1942 when the LCME was created. Recognized for its commitment to medical education, research, and healthcare excellence, WFUSM has a rich history of producing exceptional healthcare professionals and impacting care of North Carolinians in the western Carolinas. The MD program is committed to a mission of educating future physicians empowered to transform health for all and is committed to improving the health of individuals and communities through lifelong learning. The school is guided by the University’s motto, Pro Humanitate (for humanity), which anchors teaching priorities within a tradition of humanism in medicine. Below are a selection of programs including curricular and extra-curricular the promote a future physician workforce prepared for the primary care and rural health needs of all communities.
Selected Extracurricular Opportunities for WFUSM Students:
Family Medicine Interest Group: The mission of the Wake Forest University School of Medicine Family Medicine Interest Group is to encourage interest in the specialty of Family Medicine; furthering the ideal of longitudinal, patient-centered care. Inspired by the AAFP Family Physicians’ Creed and the Mission Statements of the AAFP and NCAFP, we strive to holistically improve the health of our community while exemplifying professionalism and creativity. Our overarching goal is to support and recruit interest by capturing students in training to become exceptional, humanistic physicians. Exposing students to Family Medicine as a career path early at interest fairs and via lunch talks supports this goal. Having upper-level students (formally and informally) mentor new students continues this pipeline through the residency match process. Furthermore, our events consider health care policy and affordability, striving to advance high quality clinical evidence and advocate for health equity. We look to find ways to engage with our local community through volunteering opportunities that encourage our student body to learn more about the health needs of our city. By hosting events and combining efforts with other student groups, we hope that topics (e.g. LGBTQ health and Social Medicine) that do not receive extensive attention elsewhere in the curriculum are illuminated. Increased interest in Family Medicine generated by our group has helped create a Rural Family Medicine elective and we will be incorporating a talk with the course director into our programming going forward. While we hope that our efforts lead to more students entering the primary care Family Medicine workforce, those who choose other specialties will also benefit from our diverse programming. Over 100 students have signed up on Canvas and our through our listserv; we conducted casting and OBGYN care workshops with 20-30 students; we attended NCAFP Family Medicine Day with around 18 students which is our highest turnout thus far; we have created a strong executive leadership group with eight positions including class representation, president, vice president, treasurer, event coordinators, volunteer coordinator, and AAFP liaison.
Share the Health Fair: According to the 2022 Forsyth County SCOTCH Report, the top five intervenable causes of death for the county are cancer, heart diseases, chronic lower respiratory disease, cerebrovascular disease, and diabetes. Share the Health Fair exists to help meet these health discrepancies and improve health equity in Winston-Salem by minimizing barriers to care, improving social determinants of health, increasing awareness of preventative measures to avoid common chronic diseases, connecting fair participants to options for yearround health care, and empowering fair participants with the tools necessary to take their health into their own hands. Since its inception in 2000, the mission of the Share the Health Fair has been to provide basic medical screenings and information on health care and healthy living for all members of the Winston-Salem community, especially those who may not otherwise have adequate access to these services. It is an entirely student-organized effort, providing a unique opportunity for WFUSM students to learn about community health and promote wellbeing within the community that has welcomed us as we pursue medical education. Share the Health Fair hosts over 300 attendees per year and offers several integral and highly requested services including dental care, mammography, pap smears, and vision care. The fair in 2024 was staffed by over 200 volunteers, including 166 students, 22 physician volunteers, and 42 community partner volunteers helping with services ranging from medical consults to personal hygiene product distribution and more.
Some additional statistics from the fair that you may or may not be interested in incorporating:
- 80% of participants identified as Hispanic/Latino
- 72% of participant households had incomes <$30,000
- 65% of participants have no health insurance
- 58% of participants have no PCP
DEAC Clinic: The DEAC (Delivering Equal Access to Care) Clinic is a student run physician staffed free clinic whose mission is to provide high-quality, free healthcare to the underserved patients in our community while also creating a unique service oriented-learning experience for the students of Wake Forest. Since its inception in 2008, we have been providing primary care to uninsured patients in our community every Monday night. Through our clinic, we provide a great opportunity for our students to experience primary care firsthand while also performing a vital service to our community members. While we focus on primary care, our clinic also offers multiple other services to our patients in an effort to provide holistic care. First, we offer specialty nights approximately once every other month across five specialties including orthopedics, gastroenterology, neurology, pulmonology, and dermatology. Through these specialty nights, we address gaps in the care of our patients that otherwise would not be able to be filled. We also offer two auxiliary clinics to for patients in our community; the DEAC Foot and Ankle Clinic and the DEAC Vision Clinic. The Foot and Ankle Clinic provides podiatric care and a free pair of shoes to unhoused patients in our community who desperately need it. The DEAC Vision Clinic provides free ophthalmologic care which includes free glasses and even surgery for patients who need it. Finally, through DEAC Outreach, we are able to go out into the community and screen patients for chronic diseases such as hypertension and diabetes while also increasing our visibility within the community.
In addition to these services, we also realize that providing primary care requires addressing not only our patients’ medical issues but also their social determinants of health. In order to achieve this goal, we have multiple programs aimed at closing these gaps. First, through our partnership with campus kitchen we are able to provide a meal and a produce bag for each patient who comes to our Monday night clinic. We are also currently working to expand this service for our Foot and Ankle and Vision Clinics. Recently, we have implanted a hygiene cart at our clinic stocked with soap, deodorant, toothbrushes, and many other essentials that are patients are welcome to take when they come for their appointments. Lastly, we have also began screening our patients for other needs that they may have such as transportation or help paying rent or utilities. We then use this information to refer them to local organizations that provide assistance in the particular area that they require it. Through addressing these social determinants of health, we strive to provide holistic primary care to our patients.
Programs Offered:
- Specialty Nights: The clinic hosts specialty nights across five different specialties, including Orthopedics, Neurology, Gastroenterology, Pulmonology, and Dermatology. These nights provide essential services to patients who otherwise would not have access to such care.
- Vision Clinic: This clinic offers complete, dilated eye exams and prescription glasses to patients. It also refers patients to Atrium Health Wake Forest Baptist Eye Center for further management of ocular conditions.
- Foot and Ankle Clinic: This clinic provides foot care to the homeless population, including foot exams, podiatrist visits, and distribution of foot care kits.
- Patient Navigator Program (PNP): This program connects patients with medical student volunteers who help them achieve their health goals through bi-weekly phone calls.
- Care Coordinator Role: Care Coordinators help bridge the gap between DEAC workflow and patient needs, connecting patients to healthcare access, specialty appointments, and community resources.
- Food Insecurity Project: In partnership with Campus Kitchen, this project provides meals to patients.
- Stopping Tobacco by Organizing Peers (STOP): This program offers smoking cessation therapy, including counseling and nicotine replacement therapy.
- Care Provided: The DEAC Clinic offers students an opportunity to experience firsthand a wide range of medical services, including primary care, specialty care, vision care, foot care, and smoking cessation therapy. It also provides essential medical supplies, such as prescription glasses, CPAP machines, oxygen tanks, and foot care kits.
Impact on Patients and the Community:
- Visits and Patients: From July to December 2024, the clinic had 89 total visits, serving 47 unique patients. Throughout the entire year, there were 207 visits and 96 unique patients.
- Volunteer Contributions: 126 students volunteered 274 times, and 13 preceptors volunteered 43 times during the second half of 2024.
- Specialty Nights: The clinic hosted 10 specialty nights, providing services to 26 patients across 29 visits.
- Vision Clinic: The Vision Clinic served 36 patients, ordered 16 pairs of prescription glasses, and referred 9 patients for further management.
- Foot and Ankle Clinic: This clinic served an average of 32 patients each month, providing foot care and distributing foot care kits.
- Patient Navigator Program: The program currently has 12 enrolled patients and 13 student patient navigators.
- Food Insecurity Project: Campus Kitchen donated 96 meals to patients over 16 Mondays.
Key Outcomes: The DEAC Clinic has significantly improved access to healthcare for populations in Western North Carolina. The specialty nights and various clinics have provided essential medical services that patients would otherwise not have access to. The Patient Navigator Program and Care Coordinator Role have enhanced patient care coordination and support. The clinic's outreach initiatives and public relations efforts have strengthened community engagement and awareness of its services.
- Total Visits: 89 visits from July to December 2024, and 207 visits for the entire year.
- Unique Patients: 47 unique patients served from July to December 2024, and 96 unique patients for the entire year.
- Student Volunteers: 126 students volunteered 274 times from July to December 2024, and 185 students volunteered 476 times for the entire year.
- Physician Volunteers: 13 preceptors volunteered 43 times from July to December 2024, and 16 preceptors volunteered 89 times for the entire year.
Overall, the DEAC Clinic has made a substantial impact on the health and well-being of its patients and the community, demonstrating a strong commitment to providing comprehensive and compassionate care.
Schweitzer Fellowship: The North Carolina Albert Schweitzer Fellowship is a prestigious, service-focused program that supports graduate students in implementing community-based health initiatives aimed at reducing health disparities and addressing the needs of underserved populations. Each year, Schweitzer Fellows design and carry out innovative, impactful projects in collaboration with local agencies, while also participating in interdisciplinary learning experiences that cultivate their leadership and professional development. For the 2024–2025 fellowship year, two new programs were launched under the Schweitzer Fellowship umbrella to address critical gaps in healthcare access and preventative services in North Carolina.
SEE: Screening Eyes and Education Program
The first initiative is the Screening Eyes and Education (SEE) Program, designed to address eye health disparities among underinsured and uninsured populations in the Winston-Salem area. The program’s primary objective is to provide free eye health screening events at Downtown Health Plaza (DHP) on a quarterly to monthly basis. In addition to screenings, the program offers referrals for follow-up care to those in need.
Participants at these events receive no-cost services that include basic eye examinations, referrals to free clinics, eye health education, and nutrition counseling aimed at reducing risk factors associated with eye disease.
Schweitzer fellows selected played a key role in leading the initiative. They have reported a meaningful impact from their involvement. Two participants shared: “We think the experience has made a very impactful difference on our medical careers, and we plan on continuing to work with the underserved population in the future.”
Program Outcomes to Date:
- 174 individuals were screened for eye disease
- 50 individuals (29%) were referred to free clinics for follow-up care
- 13 individuals (26% of those referred) attended their follow-up appointments
- 14 medical student volunteers were trained in performing basic eye exams
Free Foot Clinic – Shelter Health Services, Charlotte The second program is the Free Foot Clinic, housed at Shelter Health Services in Charlotte. This initiative serves women experiencing homelessness, providing essential foot care services and improving both health outcomes and quality of life.
Program Outcomes to Date:
- 116 patients received free foot care services
- 2 patients were referred to Myers Park Clinic for additional care
- All 116 patients reported applying one or more foot care techniques weekly for two months or longer
- 116 patients received a new pair of properly fitted sneakers
- 45 medical student volunteers were trained to perform foot and ankle exams
All 45 volunteers reported increased confidence and competence in providing foot and ankle care, as well as a deeper understanding of how to serve individuals experiencing homelessness.
Selected Programs within the WFUSM Curriculum:
The “Wake Ready!” curriculum provides an individualized approach to prepare students towards their medical career. It advances WFUSM’s national reputation for graduating first-rate clinicians, educators and scholars. It provides students with flexibility to explore their interests and positions graduates for outstanding performance in the top residency training programs in the nation.
Clerkships: As part of the Wake Ready Curriculum, students complete a variety of community rotations/experiences between our two campuses (Winston-Salem and Charlotte) during their clerkships, with the opportunity to participate in electives in the post-clerkship curriculum. During the clerkship curriculum, all students complete an Ambulatory Internal Medicine (IM) clerkship and Family Medicine clerkship. Students also complete ambulatory components during their Pediatrics, Psychiatry, Neurology, and Obstetrics/Gynecology clerkships. A description of the dedicated community/ambulatory clerkships of Ambulatory IM and Family Medicine are included below.
Clerkship: Ambulatory Internal Medicine
Duration: 2 weeks on the Winston-Salem campus and comparable longitudinal clerkship on the Charlotte Campus
Description of Clerkship: The core clerkship in Ambulatory Internal Medicine focuses on the basic competencies of ambulatory internal medicine and management of chronic disease. Students spend time in various ambulatory settings which include continuity care clinics, complex care teams, and urgent care clinics. Students are expected to participate in the care of patients presenting to these clinics, including but not limited to conditions such as COPD, Diabetes, Hyperlipidemia, Hypertension, Obesity, Tobacco Use, Depression, and Joint Pain. Also, as part of the clerkship, students complete a Population Health Quality Improvement (PHQI) activity. In this project, they review the charts of ten patients they have cared for to identify gaps in preventive screenings and immunizations. Students then take active steps to close these health maintenance gaps by engaging directly with the patients identified through the PHQI process.
Participants in clerkship: All third year medical students on the Winston-Salem and Charlotte campuses (approx. 145 total)
Outcomes: Participation in care of patients with the above listed diagnoses/conditions and completion of the Population Health Quality Improvement project.
Clerkship: Family Medicine
Description of Clerkship: The Family Medicine clerkship is a 4 week clerkship on the WinstonSalem campus and Charlotte campus during the 2023-2024 academic year. The clerkship consists of students participating in patient care at the outpatient family medicine clinics in both Winston-Salem and Charlotte. Students are expected to participate in the care of patients presenting with back/neck pain, dysuria, headache, joint pain, rashes, asthma/COPD, depression, diabetes mellitus, hyperlipidemia, hypertension, obesity, respiratory illness, and tobacco use. Students also participate in adult and pediatric maintenance health exams and counseling on substance cessation.
Participants in clerkship: All third year medical students on the Winston-Salem and Charlotte campuses (approx. 145 total)
Outcome: Participation in care of patients with above noted presentations, along with final exam in course (NBME exam).
Additionally, during the clerkship phase of the curriculum, students also complete the Health Equity thread/curriculum. This longitudinal curriculum encompasses a series of activities that focuses on health equity and the social determinants of health, such as housing, transportation, food insecurity, access to care, vulnerable patient populations, maternal-fetal health disparities as examples. Often, the experiences are partnered with a community organization in WinstonSalem and Charlotte that are working to address these disparities.
Longitudinal Health Equity Thread
Goals of Program:
- Understand the scope of health disparities in the United States.
- Identify ways to contribute to the reduction of health disparities as a practicing clinician.
- Demonstrate the knowledge and skills needed to improve the health of underserved populations.
- Explore activities with community partners that will foster an interest in careers working with underserved populations.
Number of participants: All third year medical students at both the Winson-Salem and Charlotte campuses (approx. 145 students)
Outcomes: Students engage with multiple community-based organizations and complete a variety of exercises throughout the curriculum that address health equity and the social determinants of health. Wake Forest medical students also have the opportunity to participate in a variety of fourth-year electives that offer robust clinical experiences in primary care. These electives provide exposure to outpatient and community-based practices across Family Medicine, Obstetrics and Gynecology, Pediatrics, and outpatient Psychiatry.
Electives that offer primary care-focused Family Medicine experiences include Rural Primary Care, Safety Net Healthcare: Bridging Gaps and Building Advocacy, and Urban Underserved Family Medicine. All Wake Forest University medical students on both the Winston-Salem and Charlotte campuses have the opportunity to participate in these electives during their fourth year.
The Rural Primary Care elective provides students with hands-on experience caring for fullspectrum Family Medicine patients, including adults, geriatrics, pediatrics, and newborns. Students rotate within rural primary care practices alongside interprofessional teams and engage in activities aimed at improving the health of the community. They gain experience in a variety of care delivery models, including virtual care, home visits, hospital care, and traditional office-based visits. Students may choose from three sites located in rural North Carolina counties.
The Safety Net Healthcare: Bridging Gaps and Building Advocacy elective combines clinical experiences in Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs) with interactive workshops, community partnerships, and didactic sessions. Students develop a deeper understanding of the rewards and challenges faced by safety net providers while building practical skills in advocacy and community engagement. This elective emphasizes healthcare systems serving Medicaid, uninsured, and underinsured populations, and focuses on advancing health equity and addressing social determinants of health. The course fosters a commitment to reducing health disparities and supporting vulnerable patient populations. The Urban Underserved Family Medicine elective immerses students in established neighborhood clinics and community settings, where they gain firsthand experience providing care to diverse, medically underserved populations. The course leverages community partnerships and local resources to demonstrate how family physicians address barriers to healthcare access and deliver culturally competent, patient-centered care. Students work alongside family physicians and interprofessional teams to provide comprehensive care, while also learning public health approaches such as Community-Oriented Primary Care (COPC). In addition, they are introduced to tools like geographic information systems (GIS) to analyze population health trends and better understand the unique needs of the communities they serve.
Appendix B
A Roadmap for a Statewide (and Nationwide) Approach to Training Primary Care Physicians Who Will Practice in Rural North Carolina
An AHEC Proposal to develop a Collaboration between NC Medical Schools
Objectives:
- Improve the supply and distribution of physicians in needed specialties in rural communities and other communities with less access to resources to create a healthy North Carolina.
- Facilitate a path into medicine for students from rural and other underserved communities who might otherwise not have been able to envision themselves as future physicians.
- Develop and extend learning opportunities across the state of North Carolina through community-based learning and relationships.
Summary:
Medical students will choose their specialty based on financial, personal, and professional goals. A medical student is more likely to choose to practice rural primary care if they are from a rural community, are trained in a rural community and are supported in practice once they locate in a rural community. A multi-pronged approach is needed to address this set of complex and important decision points. The different components of the approach are described in more detail below.
AHEC has been convening educational leaders of the two state medical schools to focus on 1) how to recruit more students who are likely to pursue careers in needed specialties, 2) how to train students in high quality rural primary care while in medical school and 3) how to create and support high functioning rural practices in which to teach students. The other components – residencies and post-training support in addition to scholarships, loan forgiveness and increased reimbursements - are also critically important and need to be addressed in a different manner. We are working together to develop a pilot Pathway to Primary Care that, once developed, could be extended to any interested North Carolina medical school and other health professional programs.
Critically Important Areas of Focus to Achieve Objectives:
To reach these objectives, the program will:
- Recruit students into medical school who are more likely to pursue careers in needed specialties in rural and other underserved communities (Linkage Programs into Medical School)
- Train these students in high quality primary care while in medical school (Rural Tracks with Focused Curriculum)
- Creation and Support of high functioning primary care practices able to effectively teach (Select Teaching Practices)
- Invest in expanded and new rural residency programs. There are opportunities to leverage state and federal partnerships and create training programs in rural communities and resident naïve hospitals to increase the access to training opportunities where people are from and where they are needed for the future workforce.
- Help students match into appropriate residencies and support them during residency training (Facilitated Primary Care Residency Training)
- Provide further support and training after residency to optimize their successful entry into practice in rural and other underserved areas (Fellowship Training Programs)
- Provide financial support during training to allow learners to focus on their training and not be burdened by debt load that dissuades them from pursuing careers in primary care with a goal of entering practice without debt (Scholarships and Loan Forgiveness Programs)
- Continue to work at a national and state level to increase financial investments in primary care to allow for long-term sustainability of primary care practices (Increase Primary Care Reimbursement)
Area of Focus #1: Linkage Programs from Undergraduate Training Programs and Post Baccalaureate Master’s Program
- Strengthen pre-health advising system at each of the 16 UNC System Schools to effectively prepare interested students for careers in medicine and other health care careers through shared resources (e.g. webinars, websites) and specific training of advisers. The focus is students who are likely to pursue careers in rural medicine.
- Develop a Pre-Health Certificate in participating UNC System Schools. The Certificate is developed in collaboration with the admissions committees of participating medical schools and holds high value in the admissions process. Focus on students who are likely to pursue careers in rural medicine.
- Collaborate with existing and evolving Master’s Program in the UNC System to offer a rigorous biomedical science core and an integrated clinical component for students with a Bachelor’s degree who have an interest in rural medicine and need additional preparation prior to applying to medical school. The value of the master’s Program is communicated to the admissions committees of participating medical schools and holds high value in the admissions process.
Key components of the program include 1) mentorship and 2) curriculum focusing on professional formation, clinical skills, and academic preparation. Universities in the UNC System will be selected based on their interest in participating and their ability to recruit students who will likely pursue careers in rural and other underserved areas.
The educational collaborative convened by AHEC will further refine these programs.
Program participants who matriculate into medical school are guaranteed a place in the Rural Track described below and will learn in high performing Select Teaching Practices in rural communities.
Area of Focus #2: Focused Curriculum with Community Health Service Track/Training:
This track would expand the total number of students engaged in rotations and experiences across rural and less resourced communities. It will also build a cohort of students who can support and grow with each other both in school and when practicing and will, hopefully, encourage more students to select rural primary care. In addition, having a specific and named rural track/training for students committed to rural practice will provide students additional leverage for residency placement through an LCME accredited track. Medical Schools participating in the collaboration will either have such a track already in existence or will develop such a track. Schools may choose to name their track differently. The components below are draft components of what such a track would include. Over the past year, the UNC SOM has incorporated many of these components in developing a Community Health Training Program. It was informed by the lessons learned from the FIRST Program (Fully Integrated Readiness for Service) and the Kenan Rural Scholars Program as well as the statewide work of the AHEC program. 24 first year medical students enrolled into the program in the Fall of 2025.
The educational collaborative convened by AHEC will further refine this area of focus.
Participating medical schools will work together to offer students an augmented rural and underserved curriculum. This will allow team formation among students who have shared commitment to education and engagement in rural and underserved communities across the state.
The track focuses on training medical students to become physicians who will serve rural and other underserved communities and will better prepare medical students and serve as a recruitment incentive for students considering careers in primary care.
Sample Program Components:
- Mentorship – Entering into Community Health Track, every student will be assigned a rural health preceptor. They will help students develop a statewide network of support that will provide important academic, professional, and social development.
- Curricular Enhancements – Students in the track will complete all core requirements of the respective medical school curricula, but in addition will learn skills essential to being a rural physician in NC such as enhanced procedural skills including advanced point of care ultrasound skills.
- Training in rural hospitals for a portion of required and elective inpatient experiences.
- Training in Select Teaching Practices for the majority of outpatient clinical experiences – Select Teaching Practices are essential to the success of this program and are currently underdeveloped at most medical schools. For this reason, Creation and Support of Select Teaching Practices is discussed as a separate area of focus.
Area of Focus #3: Creation and Support of Select Teaching Practices
Students will learn clinical medicine in teaching practices that are chosen based on the location of the practice in a rural or otherwise underserved setting, the quality of care delivered in the practice, and the high commitment to education. These practices will receive additional support and training to allow them to effectively train Track students.
The creation of high functioning primary care practices in which to teach learners (Select Teaching Practices) deserves further discussion. Developing these Select Teaching Practices is fundamental to ensuring a well-prepared primary care workforce for our future as these practices will provide learners with the skills and role modeling needed to succeed in primary care. Five such hubs have been funded to date by the NC Legislature and students are learning in those sites. Implementation of the teaching hubs is well underway and NC AHEC is at the early stage of evaluating this program.
Sample Components that make Select Teaching Practices different from currently existing community preceptors:
- Engaged Practices that provide high quality care. Select Teaching Practices are high functioning primary care offices that provide a broad range of services to patients and have an enthusiasm for passing on their knowledge to the next generation of primary care clinicians. Select Teaching Practices teach regularly so they can hone teaching skills and so that students integrate effectively into practice and directly contribute to the care of patients. Teachers in Select Teaching Practices participate in occasional events to help improve their teaching skills and help improve the curriculum. Select Teaching Practices are important members of the teaching team will have an important voice in how students are trained. The rural hubs funded by the General Assembly are required to have students from two or more professions (medical students and physician assistant or nurse practitioner student) more than half the time. They have also developed or plan to develop interprofessional practice and education.
- Select Teaching Practices are reimbursed at rates that allow them to teach effectively and remain financially viable. High performing practices face multiple pressures and increased reimbursement will allow them to compensate physicians and other staff to effectively teach students. The General Assembly funded hubs are supported by $150,000 per year.
- Select Teaching Practices teach learners from multiple health disciplines to allow for high quality interprofessional education that is needed to prepare an effective health workforce of the future.
- Students learning in these sites are incorporated into the rural communities in which the Select Teaching Practices are located. Housing is located in the communities to foster community integration and collaborative learning. Such immersive experiences are known to increase commitment to pursue careers in rural primary care. Adequate short-term housing continues to be a challenge in many communities.
- Students assigned to Select Teaching Practices intend to pursue careers in primary care. These students are carefully selected for their interest in primary care and will receive focused training in high quality primary care. Select Teaching Practices are thus able to teach a highly motivated group of students that share the practices enthusiasm for rural primary care.
- Students assigned to Select Teaching Practices make useful contributions to care. The same group of students are assigned to Select Teaching Practices over time so that they get to know the practice. This allows students to contribute to patient care in meaningful ways. The students are able to assist in value-based care, patient education, documentation, and other tasks. Lessons being learned from these sites will be used to refine the current hubs and develop proposals to expand to other communities. The educational collaborative convened by AHEC will help in this process.
Additional Areas of Focus that are important but are not currently part of this collaborative:
Facilitated Primary Care Residency Training
Participating residencies will ensure that Track students continue to receive mentorship and support during residency.
The goal of this longitudinal approach is to train students in needed specialties to work in rural and underserved communities. Formal training often ends with residency. A minority of medical students from NC medical schools will practice primary care or psychiatry, and far fewer still will practice in rural and underserved areas.
Graduate Medical Education (GME) in NC has grown from 4 communities 50 years ago to 26 communities now. Most GME outside of academic health centers is in primary care. Training residents in the communities in rural and urban communities where people live and work is a proven strategy to increase provider supply and improve access to care. Additional communitybased residencies to align with this Pathway are needed.
Students from the track will be encouraged to schedule guest rotations with aligned community-based residency programs. These students will be encouraged to consider these programs as ideal opportunities to train in the types of communities they want to live and work in and develop professional connections to those communities.
Fellowship Training Programs
Upon completion of residency, the program would support entry into practice with additional fellowship training. Fellowship training will provide enhanced clinical and business skills to succeed in rural practice. The fellowship will also provide teaching skills to grow the next generation of elite teaching practices.
MAHEC and UNC Office of Rural Initiatives have developed a rural fellowship program. Recently trained providers with employment in a rural community can have a portion of their professional time covered by the fellowship (10-20%) to allow the physician time to develop specific skills for rural practice as well as networking and rural leadership development. This fellowship has demonstrated early success and efforts will be made to expand it statewide. AHEC Practice Support can provide support to practices that employ recent graduates. Support includes assistance in areas such as practice management, quality improvement, electronic health record optimization, behavioral health integration, and workflow redesign. Ideally, these graduates could also practice in a Select Teaching Practice.
Financial Support and Reduction of Loan Burden
Loan burden on students graduating from medical school has increased dramatically over the past decade. The current average debt of graduating medical students nationally is now about $200,000. With continued wide disparities in salaries between specialties, large debt burden can influence student choice of specialties.
Programs to minimize financial pressures during training and reducing eventual total debt burden are an important part of ensuring an appropriate physician workforce in rural and other underserved communities. The goal of this program is to have participants enter practice with zero debt. Ideally, this program would align with the scholarship and loan repayment programs recently enacted by the General Assembly.
Increase Primary Care Reimbursement
Work at a national and statewide level to implement the recommendations of the National Academies of Science Engineering and Medicine to pay for primary care teams to care for people not doctors to deliver services. The report recommends that:
- Payers should evaluate and disseminate payment models based on the ability of those models to promote the delivery of high-quality primary care, not on achieving shortterm cost savings.
- Payers using a fee-for-service (FFS) model should shift primary care payment toward hybrid (part FFS, part capitated) models and make them the default over time.
- The Centers for Medicare & Medicaid Services (CMS) should increase the overall portion of spending going to primary care.
- States should implement primary care payment reform by facilitating multi-payer collaboration and by increasing the overall portion of health care spending in their state going to primary care. Implementing high-quality primary care begins by committing to pay primary care more and differently because of its capacity to improve population health and health equity for all of society, not because it generates short term returns on investment for payers. High-quality primary care is a common good promoted by responsible public policy and supported by private-sector action.
Reducing student debt and increasing reimbursement are essential components as students weigh their personal and professional goals when choosing a medical specialty.
Selected References
- Implementing High Quality Primary Care: Rebuilding the Foundation of Health Care. The National Academies of Science, Engineering and Medicine 2021. https://www.nationalacademies.org/our-work/implementing-high-quality-primary-care
Multiple Models exist on which this proposal is built. Links to some of these programs are provided below:
- Alabama College of Community Health Sciences: https://cchs.ua.edu/rural-programs/rmsp/#:%7E:text=The%20Rural%20Medical%20Scholars%20Program,where%20they%20are%20most%20needed
- Michigan State: https://msururalhealth.chm.msu.edu/programs/rural-physician-program.html
- U of Minnesota https://med.umn.edu/md-students/individualized-pathways/rural-physicianassociate-program-rpap
- NE Ohio Medical School: https://www.neomed.edu/medicine/admissions/paths/earlyassurance/
- Eight Year Continuum. Brown Rhode Island. https://plme.med.brown.edu/
- JAMP with support from Texas Legislature: https://www.uta.edu/academics/schoolscolleges/science/degree-programs/health-professions/special-programs-volunteering-researchopportunities/jamp
- WWAMI; Recruit students from rural communities and enroll them in Rural Track (TRUST). https://www.uwmedicine.org/school-of-medicine/md-program/wwami
References
- NC DHHS Office of Rural Health. Safety Net Sites website. Accessed February 27, 2025. https://www.ncdhhs.gov/divisions/office-rural-health/safety-net-resources/safety-net-sites
- Iglehart J. The challenging quest to improve rural health care. NEJM, 2018. 378(5):473–479. https://www.nejm.org/doi/full/10.1056/NEJMhpr1707176
- Paralkar N, LaVine N, Ryan S, et al. Career Plans of Internal Medicine Residents From 2019 to 2021. JAMA Intern Med. 2023;183(10):1166–1167. https://doi.org/10.1001/jamainternmed.2023.2873
-
Kind AJH, Buckingham W. Making Neighborhood Disadvantage Metrics Accessible: The Neighborhood Atlas.
New England Journal of Medicine, 2018. 378:2456–2458.
DOI: 10.1056/NEJMp1802313. PMCID: PMC6051533.
And the University of Wisconsin School of Medicine and Public Health. 2022 Area Deprivation Index 4.0.1. Downloaded from https://www.neighborhoodatlas.medicine.wisc.edu/ on February 27, 2025. - The University of Wisconsin School of Medicine and Public Health. 2022 Area Deprivation Index 4.0.1. Downloaded from https://www.neighborhoodatlas.medicine.wisc.edu/ on February 27, 2025.
Suggested Citation: Galloway E and Tilson H. Outcomes of NC Medical School Graduates: How Many Stay in Practice in NC, in Primary Care, and in High Need Areas? Program on Health Workforce Research and Policy. Cecil G. Sheps Center for Health Services Research. The University of North Carolina at Chapel Hill. April 11, 2025.